If you're reading this after another attack interrupted work, sleep, dinner, or a plan you were looking forward to, the short answer is this: migraine prevention medication may help lower how often attacks happen, how intense they feel, and how long they last. It isn't about “toughing it out” better. It's about getting out of the exhausting cycle of waiting for the next migraine to strike and treating it only after it has already started.
That shift matters because migraine is not the same as a routine headache. A migraine attack can include prodrome (early warning symptoms before pain starts), aura (temporary neurological symptoms such as visual changes), photophobia (light sensitivity), nausea, dizziness, and postdrome (the drained, foggy phase after the main attack). When attacks keep recurring, reactive treatment alone can start to feel like you're always behind.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Table of Contents
- How long does it take to know if it helps
- Will I need to stay on it forever
- What if side effects show up
- Can I combine medication with lifestyle changes
Moving Beyond Reacting to Your Next Migraine Attack
Some people arrive at prevention after months of “maybe this one won't get bad.” Others get there after they've memorized where they keep rescue medication in every bag, coat, and nightstand. Either way, living attack to attack is tiring.
Migraine prevention medication is meant to change the pattern, not just blunt the next episode. The goal is to reduce frequency, severity, and duration over time so your nervous system is less likely to tip into a full attack.
Why prevention changes the conversation
A preventive plan can feel emotionally different from acute treatment. Acute treatment asks, “What do I do now that this has started?” Prevention asks, “How do we make attacks less likely to take over your week?”
That doesn't mean one pill fixes everything. It usually means a period of trial, observation, and adjustment with your clinician. Some people do well with an older oral medication. Others need a newer targeted option. Some need medication plus better sleep regularity, less rescue-medication overuse, and clearer trigger tracking.
Practical rule: A good prevention plan is rarely about finding the “strongest” medicine. It's about finding the option you can tolerate, stick with, and evaluate fairly.
You may also hear your clinician talk about raising your migraine threshold. In plain language, that means making your brain less vulnerable to the pileup of triggers that can push an attack into motion.
When to seek immediate care
Most migraine attacks, even severe ones, aren't emergencies. But some symptoms need urgent evaluation.
Seek immediate medical care for sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury.
If your symptoms feel dramatically different from your usual migraine pattern, don't assume it's “just another migraine.”
Who Should Consider Preventive Migraine Medication
Not everyone with migraine needs a preventive medication. But many people who would benefit never get offered one, or don't realize they can ask.
A simple checklist to bring to your appointment
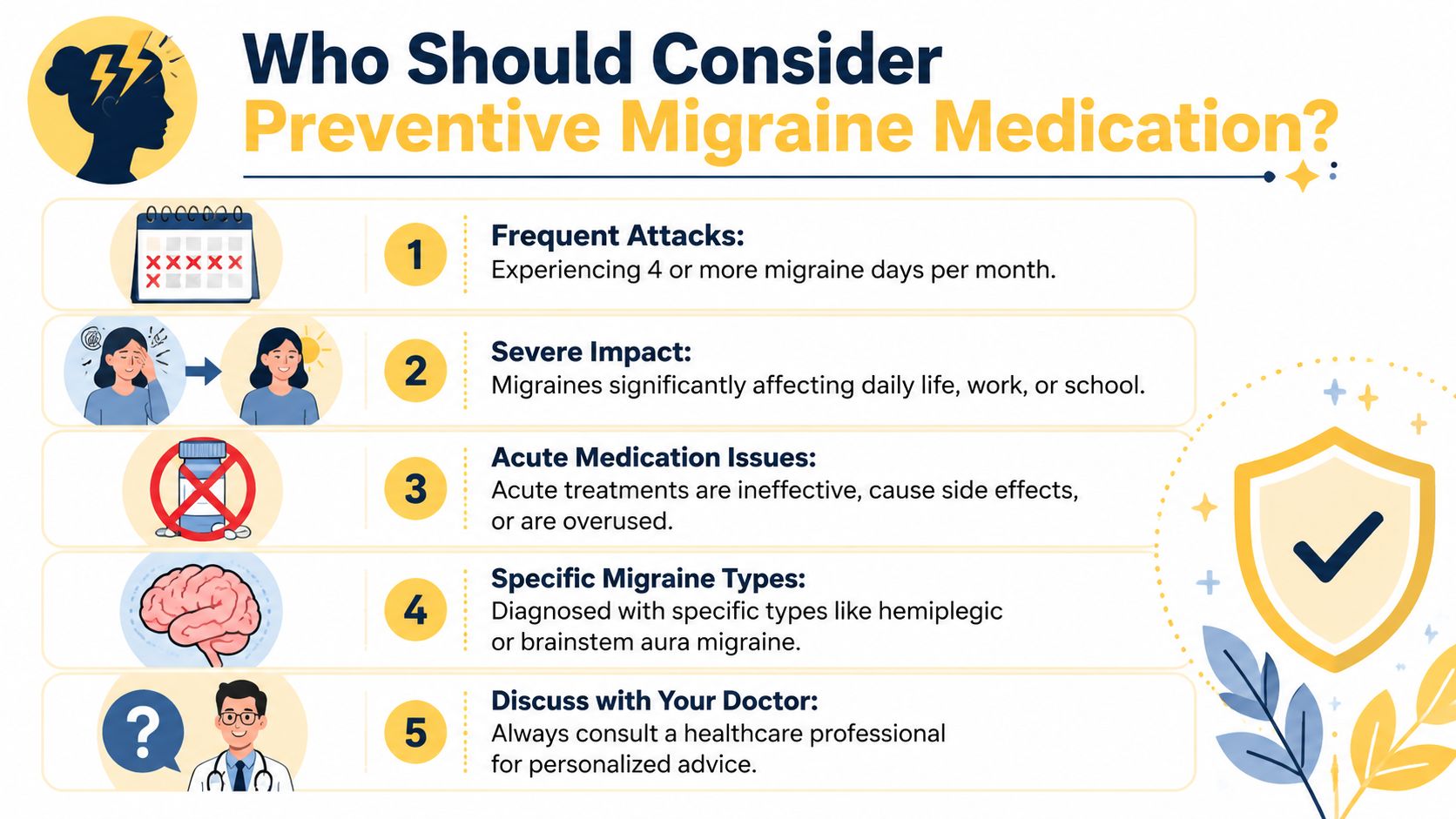
You may want to discuss prevention if any of these sound familiar:
- Frequent attacks: You have recurring migraine days each month, especially when they start shaping your schedule around “just in case.”
- Meaningful disability: Even if attacks aren't constant, they knock out work, parenting, exercise, social plans, or sleep.
- Acute treatment problems: Your rescue medication doesn't work well enough, causes side effects, or you're using it so often that it's becoming part of the problem.
- Certain migraine types: Some migraine patterns deserve especially careful planning with a clinician, including more complex presentations such as hemiplegic migraine or migraine with brainstem aura.
- A pattern of escalation: Your migraine burden is increasing, or recovery days are eating up more of your life than you expected.
The exact threshold for starting prevention varies by person. A clinician looks at more than a count. They also consider how hard each attack hits, how long you stay impaired, and what your life demands from you.
Why many eligible people never start
A lot of people assume prevention is only for severe chronic cases. That isn't true. In American Family Physician guidance on migraine prophylaxis, approximately 38% of patients with episodic migraines would benefit from preventive therapy, yet less than 13% take prophylactic medications.
That gap matters because it tells you something important. If you think, “Maybe I should have asked about this sooner,” you're far from alone.
Many people wait because they don't want to add another medication, they worry about side effects, or they think they haven't “earned” preventive care. You don't need to prove you're suffering enough to start a thoughtful discussion.
A useful question for your next visit is simple: “Based on how often these attacks affect me, do I seem like a candidate for prevention?”
A Guide to Traditional Oral Preventive Medications
Most migraine prevention medication options started out as treatments for something else. Over time, clinicians noticed they also reduced migraine attacks for some patients. That history is why migraine prevention can look confusing at first. You might be offered a blood pressure medicine, a seizure medicine, or an antidepressant even if you don't have those conditions.
A doctor's reasoning usually isn't random. It's often based on what else is going on in your health and which side effect profile fits your life best.
Beta-blockers
Beta-blockers are commonly used for heart and blood pressure conditions, but some also help prevent migraine. Propranolol is one of the best-known examples and is widely used in migraine prophylaxis, as described in this American Family Physician review.
In simple terms, these medications may help calm parts of the nervous system involved in migraine signaling. A clinician might lean toward this class if someone also has high blood pressure or certain forms of physical anxiety. On the other hand, fatigue, lightheadedness, or exercise intolerance may make this class a poor fit for some people.
If you've wondered whether related classes are ever considered, ReliefMigraine also has a guide on calcium channel blockers and migraines.
Anticonvulsants
Anticonvulsants were developed for seizure disorders, but several have strong migraine evidence. Topiramate is one of the best-established options. According to an American Academy of Neurology guideline, topiramate at doses of 50 to 200 mg/day is established as effective for episodic migraine prevention and reduces migraine frequency by 50% or more in approximately twice as many patients compared with placebo.
That sounds encouraging, but evidence isn't the same as “right for everyone.” Some people do very well with topiramate. Others struggle with side effects such as tingling, appetite changes, or cognitive slowing.
Valproic acid and divalproex are also established preventive options. The same American Family Physician review of migraine prophylaxis describes divalproex or Depakote as effective across ten clinical studies and classifies it as a Level A medication, meaning it has proven effectiveness and should be offered to patients requiring prophylaxis.
The best preventive is often the one that matches both your migraine pattern and your non-migraine life. A medication can be effective on paper and still be the wrong fit for you.
Antidepressants and other oral options
Some antidepressants, especially older ones, are used in migraine prevention because they can influence pain pathways, sleep, and brain chemicals involved in migraine biology. Amitriptyline is a familiar example.
A clinician may consider this route if sleep disruption, low mood, or certain pain conditions are part of the picture. For other people, drowsiness, dry mouth, or next-day grogginess make it less appealing.
Here's a simple overview you can scan before an appointment:
| Drug Class | Examples (Generic) | How It May Work for Migraine | Common Side Effects |
|---|---|---|---|
| Beta-blockers | propranolol | May calm nervous system activity linked to migraine | fatigue, dizziness, lower exercise tolerance |
| Anticonvulsants | topiramate, valproate, divalproex | May stabilize brain excitability involved in migraine | tingling, cognitive slowing, appetite changes, nausea |
| Antidepressants | amitriptyline | May affect pain signaling, sleep, and brain chemicals linked to migraine | drowsiness, dry mouth, weight change |
A table like this doesn't replace medical advice. It gives you better questions. If you know which side effects would disrupt your life most, tell your doctor early.
The New Era of CGRP-Targeted Therapies
Newer migraine treatments make more sense once you know one key term: CGRP, short for calcitonin gene-related peptide. This small protein plays a major role in migraine pain transmission and blood vessel changes.
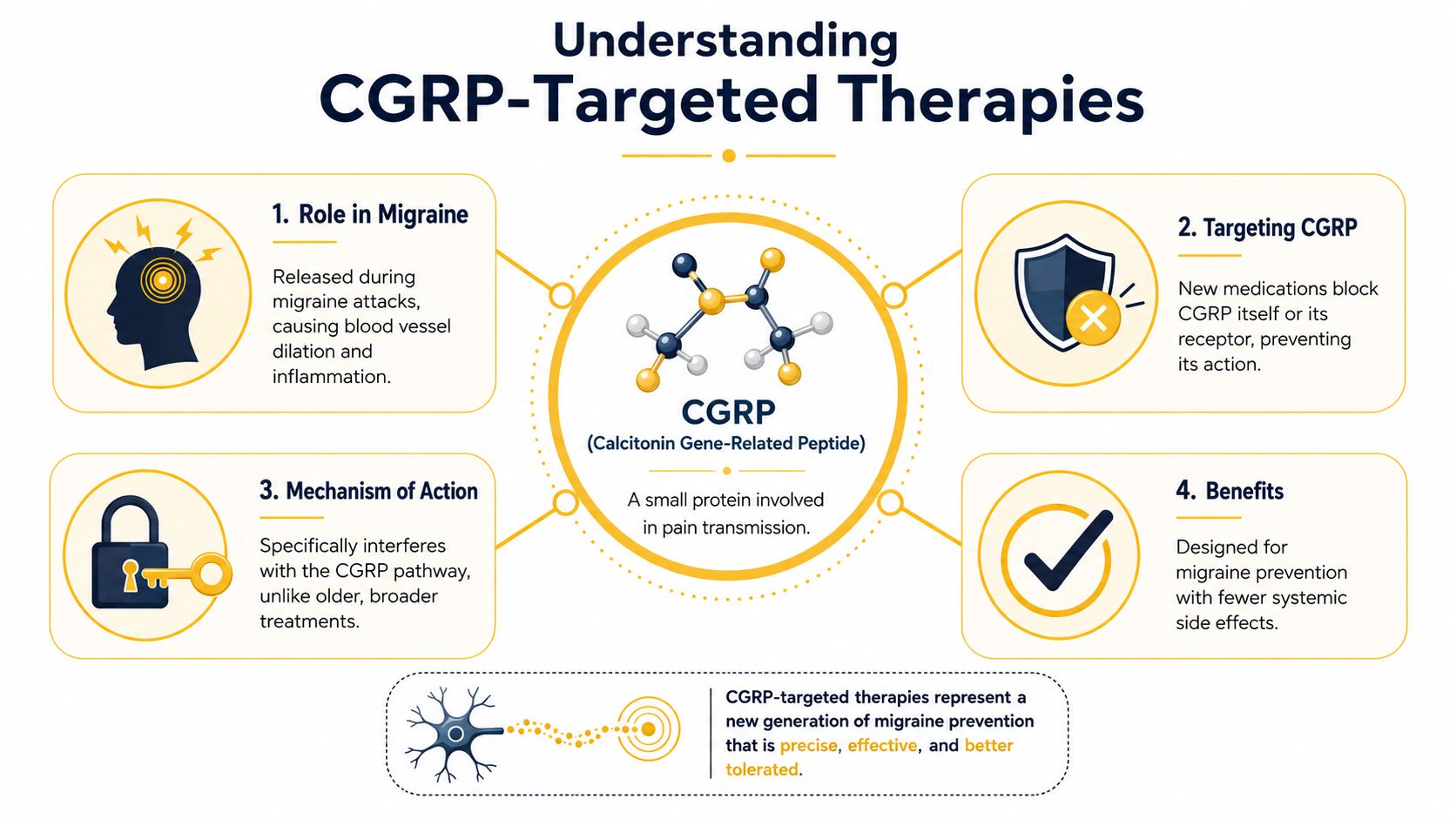
What CGRP does in migraine
During migraine attacks, the CGRP pathway is active in ways that help drive pain and related symptoms. That made it an obvious target for drug development. Instead of borrowing a medication from another field and hoping it helps migraine, researchers developed therapies aimed at this pathway itself.
This short explainer gives a useful overview of the idea in visual form.
How newer targeted treatments differ
The main preventive group here is CGRP monoclonal antibodies, often called mAbs. These include medications that target the CGRP molecule itself or its receptor. There are also gepants, which are oral CGRP-targeting medications used in migraine care.
According to the NCBI Bookshelf review on migraine medications, CGRP monoclonal antibodies represent the first class of migraine preventives explicitly developed for the disease, and network meta-analyses found efficacy comparable to traditional preventives but with significantly fewer side effects.
That doesn't mean “side-effect free,” and it doesn't automatically make them the best first choice for every patient. It does mean the conversation has changed. For many people, these drugs offer a more targeted option than older medicines that affect broader body systems.
If you want a deeper backgrounder on this treatment category, ReliefMigraine has a separate explainer on CGRP monoclonal antibody therapy.
How Your Doctor Creates Your Prevention Plan
A prevention plan usually looks less like a lightning-bolt insight and more like structured problem-solving. Your doctor is balancing migraine biology, your medical history, your daily routine, and what you can realistically access.

What your clinician weighs before choosing a medication
Many clinicians use a “start low, go slow” approach. The idea is to lower the chance of side effects while giving your body time to adjust and making it easier to spot whether the medication is helping.
Your doctor may consider:
- Your migraine pattern: How often attacks happen, how disabling they are, and whether you have aura, vestibular symptoms, or complicated presentations.
- Other health conditions: A medicine that helps one person may be a poor choice for another because of asthma, low blood pressure, mood symptoms, sleep problems, or pregnancy planning.
- Drug interactions and tolerability: What else you take matters. So does whether you can function well on a medication during work, driving, exercise, or caregiving.
- Practical realities: Access, prior authorizations, and cost affect real-world treatment just as much as pharmacology does.
Bring a medication list, a symptom log, and a one-sentence goal to your visit. “I want fewer attacks that knock me out at work” gives your clinician something concrete to solve.
Why insurance paperwork can shape the plan
One of the most frustrating parts of modern migraine care has nothing to do with science. It's paperwork. According to clinical tips on prior authorizations for migraine medications, many patients are denied insurance coverage for newer agents because they don't meet the minimum migraine-day frequency, typically 6 to 8 days per month, required by insurers, even if they've taken older preventive meds for years at max doses.
That can feel personal, but it often isn't. It usually reflects plan rules rather than your doctor's opinion of whether the treatment makes sense.
Detailed documentation helps. If your records clearly show frequency, prior medication trials, side effects, and functional impact, your clinician has a stronger case when approval is needed.
Is It Working? Tracking and Adjusting Your Treatment
Once you start a preventive medication, the most valuable thing you can do is track what changes. Memory is unreliable when you're exhausted, in pain, or trying to compare this month to three months ago.
A good migraine log doesn't need to be fancy. It needs to be consistent.
What to track between visits
Write down enough detail to answer one question truthfully: “Am I better than I was before I started this?”
Useful items to track include:
- Attack frequency: How many migraine days you had.
- Duration: Whether attacks are ending faster or dragging on.
- Severity: A simple rating is often enough if you use it consistently.
- Acute medication use: How often you needed rescue treatment.
- Associated symptoms: Aura, nausea, photophobia, phonophobia, dizziness, neck pain, or postdrome.
- Context: Sleep disruption, menstrual timing if relevant, stress shifts, travel, skipped meals, and environmental conditions.
A paper diary can work. A digital log can make pattern spotting easier, especially if you want a ready-made format. If you need a starting point, this migraine log template gives you a simple structure to follow.
How pattern tracking improves follow-up appointments
The smartest tracking goes beyond “I had a migraine.” It helps you connect attacks to timing, triggers, and the conditions around them. A trend in headache medicine emphasizes proactive, data-driven forecasting that blends health logs with local weather and air quality to predict risk, as discussed in Practical Neurology's review of underrepresented populations and care considerations in headache medicine.
That matters because triggers aren't universal. Humidity, barometric pressure shifts, pollen, poor air quality, disrupted sleep, or bright light may matter for you, but not for someone else. When you bring those patterns to a follow-up, the appointment gets sharper.
“It helps a little” is hard for a clinician to act on. “My migraine days are less severe, but weather-shift days still break through” is much more useful.
Tracking also helps you notice hidden wins. Maybe the number of attacks hasn't changed much yet, but the attacks are shorter, your nausea is milder, or you need less rescue medication. Those are meaningful clues when deciding whether to stay the course or adjust.
Common Questions About Migraine Prevention
A few questions come up in almost every first prevention conversation. Straight answers help.
How long does it take to know if it helps
Preventive medications usually need time. You're not judging whether it worked after a few days. Your clinician will often want a fair trial before deciding whether the medication is helping enough.
Keep expectations realistic. Improvement can show up as fewer migraine days, milder symptoms, shorter attacks, or less need for acute medication.
Will I need to stay on it forever
Not necessarily. According to Migraine Canada's overview of preventive treatments, preventive migraine medications, when taken for 8 to 12 months, reduce migraine frequency by 50% in 50% of patients, and after that period tapering may be attempted. The purpose is to raise the brain's migraine threshold so you're less vulnerable to triggers.
Some people stay on treatment longer. Others try tapering after a stable stretch. That decision should be planned with your clinician, not done abruptly on your own.
What if side effects show up
Tell your doctor. Don't just stop a prescription suddenly unless you've been specifically instructed to do that.
Side effects don't always mean failure. Sometimes they fade. Sometimes a slower titration helps. Sometimes they signal that this medication isn't your match, which is useful information too.
Can I combine medication with lifestyle changes
Yes. In fact, that combination often makes the most sense. Regular sleep, hydration, meal timing, movement, stress management, and trigger awareness can support medication rather than compete with it.
Prevention works best as a partnership. Your clinician brings medical judgment. You bring the day-to-day data that shows what your migraine life looks like.
Relief can support that partnership by helping you track symptoms, medications, and environmental patterns in one place, so your next doctor visit is based on clearer evidence instead of guesswork.