CGRP monoclonal antibody treatments are the first medications designed specifically to prevent migraine by blocking a key protein involved in migraine attacks. There are four FDA-approved options, and they offer a different path for people who haven't gotten enough relief from older preventive treatments.
If you're reading this, there's a good chance you're tired of trying medications that were originally made for something else, only to end up weighing side effects against partial relief. That's a common place to be with migraine care. A CGRP monoclonal antibody can feel different, not because it's a miracle, but because it was built around migraine biology instead of borrowed from another condition.
These medications are preventive treatments, not rescue drugs. That means the pertinent question isn't "Will this stop an attack today?" It's "Will this make my next month more livable?" For many people, that's the question that matters most.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Table of Contents
What Are CGRP Monoclonal Antibodies and How Do They Work
Finding a migraine preventive that effectively helps can be draining. Many people spend years trying one option after another, only to hear that they need to "give it more time" while they keep losing workdays, sleep, and plans.
A CGRP monoclonal antibody is different because it was developed specifically for migraine prevention. According to the Migraine Disorders explanation of CGRP-targeted treatments, these became the first migraine-preventive drugs designed specifically for the disease.
Why this treatment feels different
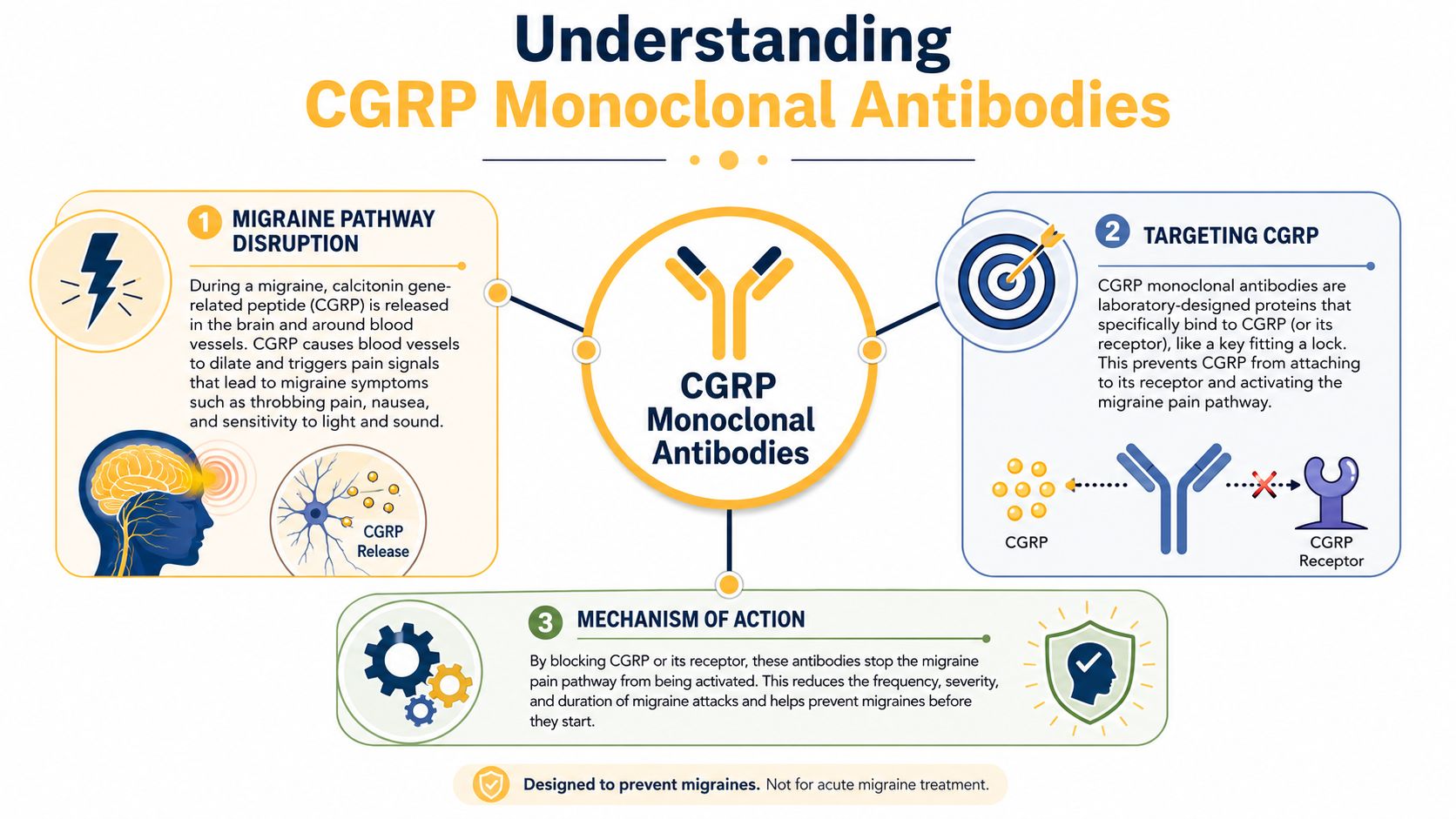
CGRP stands for calcitonin gene-related peptide. You don't need to memorize the name. What matters is that it's part of the pain signaling involved in migraine.
Think of CGRP as a messenger that helps turn up the migraine signal. If that messenger can't do its job, the attack pathway is harder to sustain. That's the basic idea behind these medications.
Practical rule: Preventive treatment is about lowering the number and burden of attacks over time, not stopping a migraine already in progress.
These drugs are also more targeted than many older preventives. A pharmacology review on CGRP monoclonal antibodies in migraine explains that erenumab binds the CGRP receptor, while fremanezumab, galcanezumab, and eptinezumab bind the CGRP ligand itself. The same review notes that these are long-acting biologics with low drug-drug interaction potential because they aren't cleared by hepatic metabolism or renal excretion.
A simple way to picture the mechanism
There are two main ways these medications interrupt the pathway:
- Blocking the messenger: Some attach to the CGRP molecule itself before it can act.
- Blocking the docking site: One attaches to the receptor, which is the place CGRP would normally latch onto.
A simple analogy helps. One approach is like catching the key before it reaches the door. The other is like covering the lock so the key can't get in.
That doesn't mean every person responds the same way. Migraine isn't one-size-fits-all. But it does explain why this treatment class has changed the conversation for people with episodic migraine, chronic migraine, with aura or without aura, and other migraine patterns that haven't responded well to older options.
The Approved CGRP Antibody Treatments for Migraine
When people hear "CGRP antibody," it can sound like one medication. It is a group of treatments with similar goals and slightly different practical details.
The four available treatments
There are four FDA-approved CGRP monoclonal antibodies used in migraine prevention:
| Comparison of Approved CGRP Monoclonal Antibody Treatments | ||
|---|---|---|
| Medication (Brand Name) | Administration Method | Dosing Schedule |
| Erenumab (Aimovig) | Subcutaneous injection | Monthly |
| Fremanezumab (Ajovy) | Subcutaneous injection | Monthly or quarterly |
| Galcanezumab (Emgality) | Subcutaneous injection | Monthly |
| Eptinezumab (Vyepti) | Intravenous infusion | Every 3 months |
The practical details above align with the Migraine Disorders overview of CGRP monoclonal antibodies, which also notes that these treatments are preventive rather than acute and are often judged after a 12-week trial period.
What daily life with each option can look like
For many, the biggest difference isn't the molecule. It's the routine.
If you prefer treatment at home, the self-injected options may feel more manageable. If you'd rather have a scheduled clinic visit every few months and not handle self-injection, an IV option may fit better.
Some practical questions to ask your clinician include:
- How comfortable are you with injections: Some people don't mind a monthly self-injection. Others strongly prefer infusion-based care.
- What does your schedule allow: A clinic appointment every few months works well for some jobs and family routines, but not for all.
- What does your insurance cover: Coverage rules often shape the choice in practice as much as medical preference.
The best option is often the one you can realistically access, tolerate, and stick with long enough to judge fairly.
Effectiveness and Timelines What to Realistically Expect
Individuals don't ask whether a preventive is perfect. They ask whether it will give them enough of their life back to matter.
What counts as success
In a 2024 prospective study of CGRP monoclonal antibodies, 5,818 patients were followed, and more than half achieved a 50% or greater reduction in monthly headache days. That's a meaningful result because migraine improvement often shows up as fewer attacks, fewer lost days, and less time spent recovering in the postdrome, which is the drained or foggy phase after an attack.
For someone with frequent migraine, a 50% reduction can be the difference between constantly rearranging life and having some predictability again. It doesn't mean migraine is gone. It means the burden may become more manageable.
The same study also found that a 30% reduction can be a meaningful early threshold in harder-to-treat groups, especially people with chronic migraine or high-frequency episodic migraine who had already failed preventive therapy. That's important because many patients dismiss early progress if it isn't dramatic.
How long should you give it
These medications are usually judged over a 12-week period rather than after the first dose. Some people do notice improvement quickly, sometimes even within the first week, as described by the earlier Migraine Disorders resource, but many treatment decisions still rely on that longer assessment window.
Here's a realistic way to think about the timeline:
- Early weeks: You may notice no change, a subtle drop in attack intensity, or a small shift in frequency.
- By the first few months: Patterns become easier to judge. This is when you and your clinician can compare baseline migraine days with current migraine days.
- After a fair trial: The decision usually becomes clearer. Continue, switch, or rethink the plan.
Don't judge a preventive only by your hardest week. Judge it by your pattern over time.
A useful mindset is to look for trends, not perfection. A treatment can be worth continuing even if you still need acute medication sometimes, still have breakthrough attacks, or still have migraine symptoms like light sensitivity and nausea during some episodes.
Side Effects and Long-Term Safety Considerations
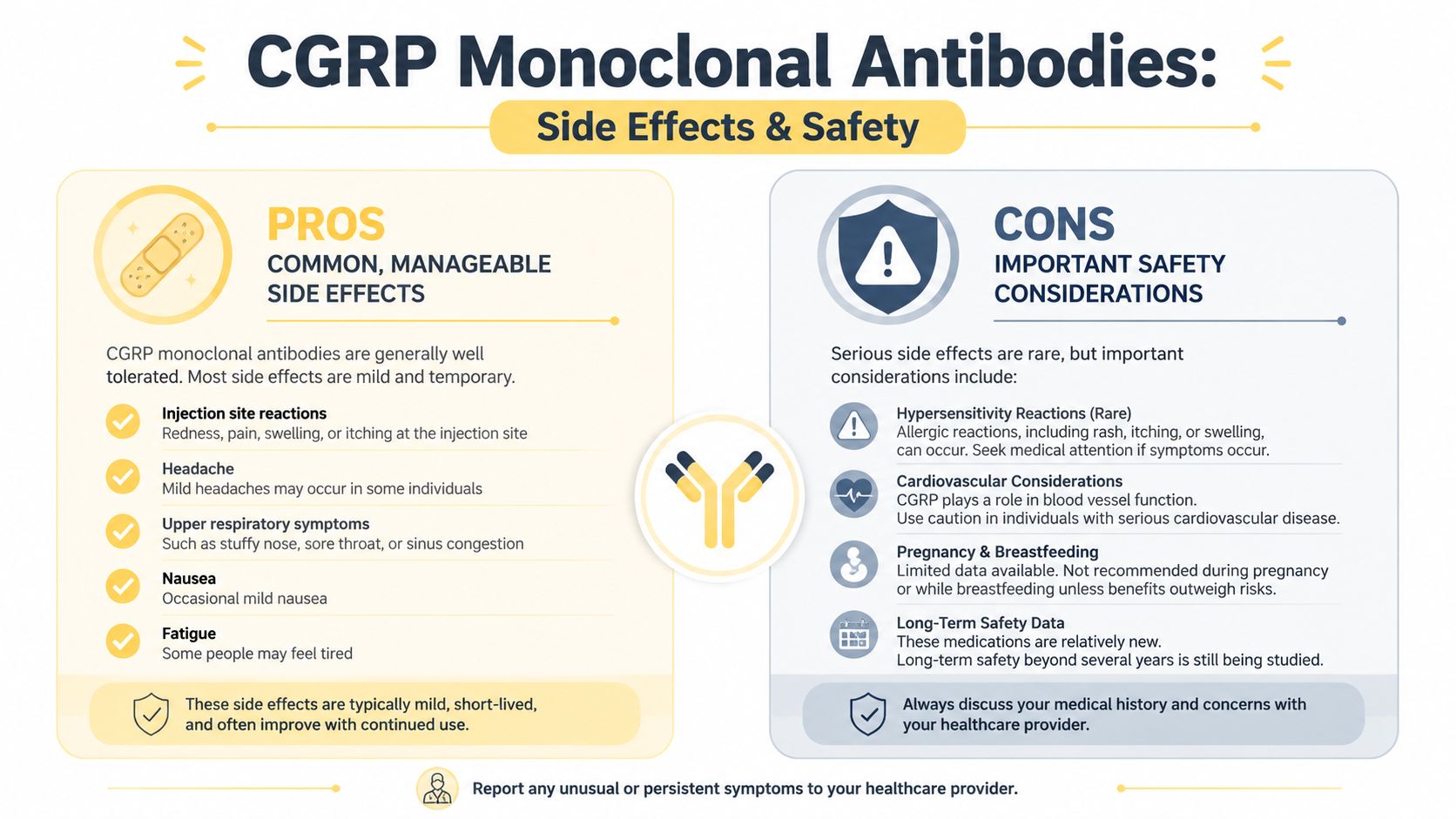
One reason people are interested in this class is that CGRP monoclonal antibodies are generally described as well tolerated. That's encouraging, but it's not the same as saying there are no tradeoffs or no unknowns.
Common issues people ask about
Public-facing migraine organizations note that side effects can include constipation, and that this may show up more clearly in real-world use than it did in clinical trials. The Migraine Canada discussion of CGRP monoclonal antibody risks and side effects also highlights rare allergic reactions and questions around vascular and gastrointestinal comorbidity.
People often ask whether these medications are "safe for the body." The honest answer is nuanced. Short-term tolerability looks reassuring for many patients, but long-term questions are still being worked through.
If you're already worried about medication side effects, it can also help to compare concerns across treatment classes. This overview of Nurtec side effects and weight changes gives one example of how patient questions often differ across newer migraine treatments.
The long-term questions that still matter
The biggest unanswered issue is long-term safety beyond the first few years. Migraine Canada notes unresolved questions about 10-year risks, especially in people with vascular or GI conditions, and mentions rare worsening of Raynaud's symptoms in some cases.
That doesn't mean these medications are unsafe. It means medicine is still collecting longer-horizon data. For patients, that distinction matters.
A newer nuance is that studies are exploring biologic effects beyond migraine prevention. Migraine Canada discusses a retinal imaging study in which ocular perfusion parameters improved and retinal structural measures changed significantly after 6 months of anti-CGRP monoclonal antibodies. That doesn't automatically translate into harm or benefit for a given person, but it does remind us that targeted migraine therapy can still have body-wide effects worth monitoring.
If a treatment helps your migraine but raises new symptoms that feel unusual for you, don't dismiss them just because the drug is called "targeted."
When to call your doctor
Contact your healthcare team promptly if you notice:
- New severe constipation: Especially if it becomes persistent or disruptive.
- Possible allergic symptoms: Such as swelling, rash, or symptoms that feel more than mild irritation.
- Worsening circulation-type symptoms: For example, concerning color or temperature changes in fingers or toes if you already have Raynaud's or vascular issues.
- Any symptom that feels clearly new after starting treatment: Even if it's not listed on a handout.
Seek immediate medical care for sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury. Those are red flags and shouldn't be assumed to be migraine.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Are You a Good Candidate for CGRP Antibody Treatment
This is usually the part people want answered most plainly. A CGRP antibody may be worth discussing if migraine is happening often enough to disrupt your life and older preventive options haven't worked well or weren't tolerable.
Signs this may be worth discussing
You may want to bring this treatment up with a clinician if these points sound familiar:
- Your migraine is frequent or disabling: Even if the exact pattern varies from month to month.
- You've tried preventive treatments before: But they didn't help enough, caused side effects, or were hard to stay on.
- You're losing too much function: Work, caregiving, sleep, exercise, social plans, and recovery time all count.
- You want a preventive option built for migraine: Rather than another repurposed medication.
Doctors also look at the full picture. That includes your migraine diagnosis, whether you have aura, how often you use acute medication, other medical conditions, and whether there are signs of medication overuse headache.
A useful appointment is usually built on records, not memory. Bring a short list of:
- migraine days
- headache days
- acute medications used
- side effects from past preventives
- questions about injections, infusions, pregnancy planning, or comorbid conditions
Insurance and access in the real world
Access can be frustrating even when a treatment makes medical sense. Insurance plans often ask for documentation, prior authorization, or evidence that you've already tried other preventive medications.
That process goes more smoothly when you prepare:
- Bring a treatment history: Write down what you've tried and why it was stopped.
- Use consistent terminology: "Migraine days per month" is often more useful than "I get them a lot."
- Ask the office how appeals work: Staff often know the wording insurers want.
- Request copies of denials and approvals: Paperwork matters if you need to resubmit.
A strong migraine diary can help your doctor show not just that you're suffering, but how often, how severely, and with what functional impact.
If cost is part of the conversation, ask about manufacturer support programs, infusion center billing questions, and whether a different administration method changes coverage. Those details can shape the path forward as much as the clinical discussion.
How CGRP Antibodies Compare to Other Migraine Preventives
The simplest comparison is this. Older preventive medications were often borrowed from other fields. CGRP antibodies were developed around migraine itself.
How they differ from older preventive drugs
Many traditional preventives come from categories like blood pressure medications, antidepressants, or anti-seizure drugs. They can help some people, and many patients still do well on them. But they were not originally built to target migraine biology.
A CGRP monoclonal antibody stands apart because it focuses on a pathway linked directly to migraine. That targeted design is a major reason people and clinicians see this class as an important shift in care.
There are also practical differences:
- How they're taken: These are injections or infusions, not daily pills.
- How they're processed: As noted earlier, they have low drug-drug interaction potential.
- What success looks like: The aim is prevention over time, not immediate rescue.
Where gepants fit in
You may also hear about gepants, which also target the CGRP pathway. The main high-level difference is that monoclonal antibodies are large-molecule biologics, while gepants are small-molecule drugs.
For patients, that often translates into different routines and different prescribing decisions. Some CGRP-targeting treatments are used preventively, some are used acutely, and some can be used in more than one way depending on the product and the clinical context. That's why it's worth asking not just "Does it target CGRP?" but "Is this meant to prevent attacks, treat attacks, or both?"
Tracking Your Progress and Answering Your Questions
You start your first CGRP antibody, and six weeks later your doctor asks, "Is it helping?" That sounds simple until you realize migraine memory is slippery. The worst attacks stand out, the milder ones blur together, and a stressful month can make any treatment look better or worse than it is.
Tracking gives you a more honest answer. It also helps with practical problems that come up outside a clinical trial, such as insurance renewals, dose changes, or deciding whether to stay the course a little longer.
Common questions people have after starting
Can I still use my acute medication?
Often, yes. A preventive and an acute treatment are commonly used together. Your prescriber should confirm which options are safe and how often you should use them.
What if it seems to work at first, then less later?
Check your diary before assuming the medicine stopped working. Migraine patterns can shift with sleep loss, stress, hormone changes, illness, weather, or frequent use of acute medication. Sometimes the treatment is still helping, but life got louder around it.
Will it help medication overuse headache?
It can be part of the plan, but it usually is not the whole plan. If acute medicines are being used often, your clinician may also talk with you about limits, tapering, and safer rescue strategies.
Does a partial response still count?
Yes. Fewer migraine days matter, but so do shorter attacks, lower pain intensity, better response to rescue medication, and getting more of your normal life back.
A treatment does not need to create a perfect month to be useful.
How long should I give it before judging it?
That depends on the medication and your doctor's plan, but in practice it usually takes more than one injection to judge fairly. A single good or bad month rarely gives the full picture.
Why does tracking matter for insurance?
Insurers often want proof that a medicine is helping before they continue coverage. A clear log of migraine days, disability, and rescue medication use can make follow-up visits and prior authorization paperwork much easier to handle.
What to track so you can judge whether it is working
Keep it simple enough that you will do it. A migraine diary should work like a blood pressure log. It does not need to be fancy. It needs to be consistent.
For the first few months, track the same core details:
- Frequency: Number of migraine days and headache days
- Severity: Mild, moderate, or severe is enough for many people
- Duration: Approximate start and stop times
- Symptoms: Aura, nausea, vomiting, light sensitivity, sound sensitivity, dizziness, brain fog, and postdrome
- Acute medication use: What you took and whether it helped
- Function: Whether you could work, read, drive, exercise, care for family, or socialize
If you want a structured format, this migraine log template gives you a practical starting point.
A short video can also make the tracking process easier to visualize.
Bring those records to follow-up visits. The question is whether it's working for you, in your actual life, not just on paper. The goal is to have a clear before-and-after picture you and your clinician can review together.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Relief can support that process by helping you log attacks, symptoms, medications, and possible trigger patterns in one place, so your next treatment follow-up is based on recorded patterns instead of guesswork.