When considering greater occipital nerve block migraine treatment, individuals are probably not casually curious. They are likely tired, foggy, and trying to figure out whether one more option is worth their time. The short answer is yes, for some people it can help. A greater occipital nerve block is an injection of local anesthetic, sometimes with a corticosteroid, placed near a nerve at the back of the head to reduce migraine frequency and pain.
What makes this treatment confusing is that it sits in an in-between space. It isn't a cure, and it isn't always a one-time fix. But it can be a practical tool when migraine has become frequent, stubborn, or hard to control with your current plan.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.

If you've already tried preventives, rescue treatments, diet changes, sleep routines, and are even looking into migraine clinical trials and emerging treatment paths, this is the kind of option that often comes up next. What matters most is setting realistic expectations before you walk into the appointment.
Table of Contents
- What studies show in plain language
- Why clinicians often use it as a bridge
- What the evidence still does not answer well
When You've Tried Everything for Migraine
There comes a point where another pill organizer, another dark room, and another “have you tried drinking more water?” comment starts to feel insulting. If that's where you are, it makes sense that you're looking at procedures instead of just another medication change.
A greater occipital nerve block usually enters the conversation when migraine has become hard to interrupt. That may mean frequent attacks, pain that seems to keep reactivating, or a pattern where one attack blends into the next and you never fully reset. People often hear about it from a neurologist, pain specialist, headache clinic, or someone else with migraine who says, “It helped me for a while.”
Why this option gets attention
What draws people to it is simple. It targets a specific pain pathway instead of working through the whole body. For someone who has dealt with medication side effects, nausea, brain fog, or limited treatment choices, that can sound like relief in more ways than one.
A lot of the appeal is practical too:
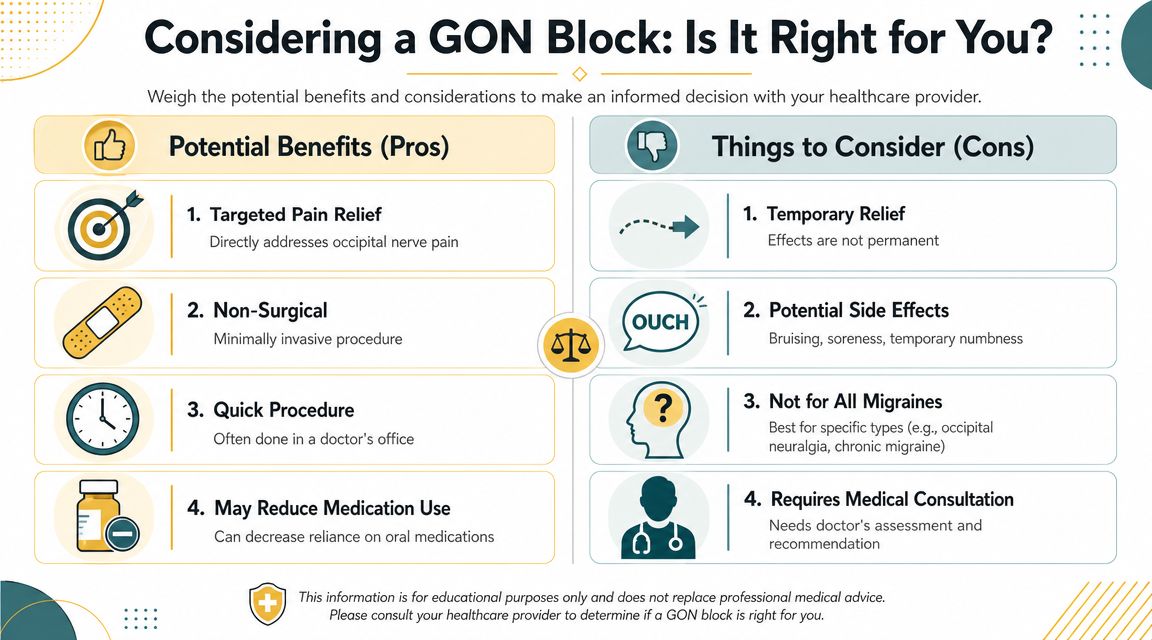
- It's quick: The procedure is usually done in a clinic setting rather than an operating room.
- It's targeted: The injection goes near the greater occipital nerve at the back of the head.
- It may work fast: Some people feel change the same day, though the pattern and duration vary.
Practical rule: A GON block makes the most sense when you're asking not just “Can this reduce pain?” but “Can this interrupt the cycle I'm stuck in?”
What people often misunderstand
Many readers come in with one of two assumptions. Either they think a nerve block is extreme and risky, or they think it's a near-guaranteed reset button. Neither view is quite right.
This is a minimally invasive procedure, but it's still a medical intervention with trade-offs. And while it can reduce migraine burden, it doesn't work equally well for everyone, and the relief window can be short for some people.
That uncertainty is one reason people spend so much time reading about it. You want to know whether it's a rescue option, a temporary bridge, or something worth repeating. Those are the right questions.
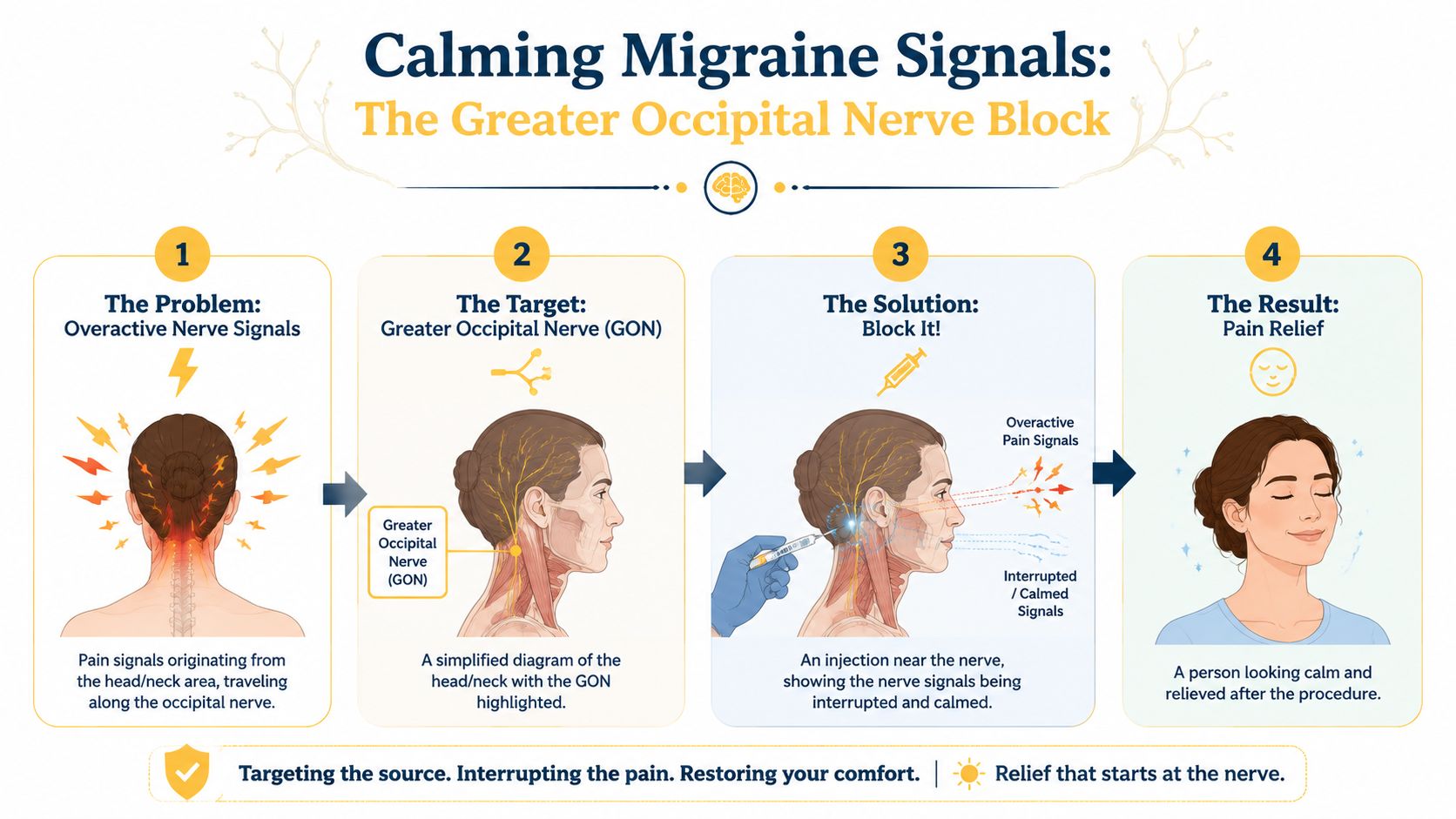
How a GON Block Works to Calm Migraine Signals
The greater occipital nerve is a nerve near the back of your head that helps carry pain information from the scalp and upper neck. In people with migraine, especially when attacks are frequent, that area can become part of an overactive pain network. A GON block aims to quiet that network down.
Why the nerve at the back of the head matters
Think of the greater occipital nerve as one of the roads carrying danger signals into a sensitive traffic system. In migraine, that system can start reacting too strongly. Signals from the back of the head and neck may feed into the broader pain response, especially in people who notice tenderness or pulling pain around the base of the skull.
That doesn't mean migraine is “just a neck problem.” It means pain pathways can overlap. For some people, calming input from this nerve seems to reduce the whole attack pattern.
What the injection is actually doing
According to procedural guidance in StatPearls on greater occipital nerve block, the block is performed by injecting a local anesthetic with or without corticosteroid near the nerve to interrupt pain transmission and reduce inflammation. The same guidance notes that relief can begin within 20 to 30 minutes and may last from hours to months.
The two parts of the injection often get lumped together, but they do slightly different jobs:
| Part of the injection | What it's meant to do |
|---|---|
| Local anesthetic | Temporarily interrupts the pain signal and may help break a pain cycle quickly |
| Corticosteroid | May add a longer anti-inflammatory effect in some protocols |
Here's the simplest way to think about it. The anesthetic is the fast-acting quiet switch. The steroid, when used, is meant to support a longer calming effect. But the best injectate mix still isn't fully standardized across migraine care.
Later in the appointment, some clinicians may use imaging while others rely on anatomy they can feel with their hands. That same procedural guidance describes ultrasound-guided techniques using landmarks such as the occipital protuberance, mastoid process, and occipital artery to improve targeting and help avoid vascular injury.
A quick visual can help if you're trying to picture what's happening inside the pain pathway:
You're not trying to numb your whole head. The goal is to calm one important input into a migraine system that may have become overreactive.
The Evidence for Using GON Blocks in Migraine Care
You get the injection, wait, and then the main question starts pressing on you. Will this buy you a few calmer days, a few calmer weeks, or almost no change at all? That gap between early relief and lasting relief is where the evidence matters most.
The research on greater occipital nerve blocks is encouraging, but it leaves some very practical questions only partly answered. Studies suggest this treatment can reduce migraine frequency and pain intensity for some people, especially in the short term. What the studies do not settle very well is who gets the best response, how long that response lasts in everyday life, and whether one injection method clearly outperforms another.
What studies show in plain language
A pooled analysis on PubMed examined 417 patients with migraine and found that greater occipital nerve block reduced headache frequency by a mean of 3.6 headache days per month compared with control, and lowered pain scores by 2.2 points. That is meaningful if your month has started to feel organized around the next attack.
The catch is timing. Much of the published research looks at early outcomes, often over a matter of weeks rather than many months. So the evidence is better at answering, “Can this calm things down soon?” than, “Will this keep helping me through the season?”
That difference matters for expectations.
Some smaller clinical reports describe larger improvements, but those numbers are harder to generalize across all patients because protocols differ. The injectate can differ. The use of steroid can differ. The technique can differ. Follow-up can differ. If you have ever read two hopeful summaries online and wondered why they do not line up perfectly, that inconsistency is part of the reason.
One useful way to read the evidence is to separate two questions that often get blended together:
- Can a GON block help during an active rough stretch? The evidence says yes, for some patients.
- Is it a lasting stand-alone fix for chronic migraine? Current evidence does not support expecting that for many patients.
- Can researchers already predict exactly who will respond best? Not very well.
That last point is frustrating, but important. A person with chronic migraine, scalp tenderness, and pain radiating from the back of the head may sound like an ideal match in theory. In practice, response still varies.
Why clinicians often use it as a bridge
Many headache specialists use a GON block as a bridge treatment. That means it may create a quieter window while another part of your plan catches up, such as a preventive medication, recovery from status migrainosus, or a reset after weeks of frequent attacks.
For a patient, bridge treatment means something very concrete. The goal may be less “end migraine for good” and more “get me out of this spiral so I can function again.”
As noted earlier, published reviews have found short-term benefit, and repeat injections are sometimes used when relief fades. That pattern helps explain why this procedure is often framed as temporary support rather than a one-time cure. If you are sorting out whether your condition meets the usual threshold for long-term preventive planning, this guide to the definition of chronic migraine can help put the conversation in context.
What the evidence still does not answer well
Patients usually want three specific answers.
Who tends to do best?
Research gives clues, but not a clean formula. Some clinicians suspect better odds when symptoms include the back of the head or upper neck, but study designs are too mixed to turn that into a reliable promise.
How long does relief last?
The honest answer is that it varies a lot. Some people get brief relief. Some get weeks. Some need repeat procedures if the first one helps but fades.
Does technique change results in a big way?
Technique probably matters for accuracy, comfort, and avoiding nearby blood vessels. But the research still does not give patients a simple rule like “this one method lasts twice as long.” Real-world trade-offs exist, and they are often discussed more clearly in the clinic than in published trials.
A better expectation is not “This will solve my migraine.” A better expectation is “This may reduce the volume of a flare, and then we see how durable that effect is for me.”
That may sound less dramatic than some online claims. It is also closer to how this treatment is typically used.
Is a Greater Occipital Nerve Block Right for You
General information concludes, and a real medical conversation begins. A GON block isn't something you “qualify” for by internet checklist alone. But there are patterns that make it more reasonable to ask about.
People who may want to ask about it
This option often comes up for people with chronic migraine, especially when attacks are frequent enough that the nervous system seems stuck in a constant state of irritation. If you aren't sure what counts as chronic migraine, this plain-language guide to the definition of chronic migraine can help you prepare for that discussion.
It may also come up when the pain pattern includes the back of the head, upper neck, or scalp tenderness around the occipital area. Some clinicians also consider it when medication choices are limited, when side effects are becoming a major barrier, or when someone hasn't gotten enough relief from several other approaches.
A practical way to think about good candidates is this:
- People with a clear pain pattern in the back of the head or neck may have symptoms that line up well with the target area.
- People stuck in a prolonged flare may be looking for interruption rather than a forever fix.
- People who need a more localized option may prefer a procedure that doesn't rely on daily medication exposure.
When it may not be the right fit
Some situations make a GON block less appropriate or require extra caution. Examples include infection at the injection site, a known allergy to a planned medication in the injection, or medical issues that affect bleeding risk. Those decisions belong with the clinician performing the procedure.
The larger issue is expectation. A review on PubMed discussing occipital nerve stimulation and block evidence gaps notes that the benefit window is variable, ranging from hours to several months, and that the most useful unanswered question is for whom, for how long, and how often it should be repeated.
That variability changes the whole decision.
| Question to ask yourself | Why it matters |
|---|---|
| Am I hoping for temporary relief or permanent control? | GON blocks are usually framed as temporary support, not a cure |
| Does my pain often involve the back of my head or upper neck? | The treatment is most directly aimed at that region's nerve pathway |
| Can I handle repeat visits if it helps but wears off? | Some people need repeat injections rather than one-and-done treatment |
If you'd feel disappointed by anything short of long-term remission, this may be emotionally harder than it looks on paper.
That doesn't mean you shouldn't consider it. It means the best candidates usually go in understanding that a positive response may still be temporary.
What to Expect During the Procedure and Recovery
The procedure itself is usually much less dramatic than people fear. Most appointments are brief, and the hardest part is often the anticipation.
What the appointment usually feels like
You'll usually sit or lie in a position that lets the clinician access the back of your head. They locate the area either by touch using surface landmarks or, in some settings, with ultrasound. The skin is cleaned, the spot is identified, and the injection is given near the greater occipital nerve.
What does it feel like? Usually a pinch, some pressure, and sometimes a brief burning sensation as the medication goes in. After that, some people notice numbness or heaviness in the scalp, while others mainly notice soreness where the needle went in.
Common short-lived effects described by The Migraine Trust's patient guidance on GON block injections include injection-site pain, swelling, dizziness, or lightheadedness.
Landmark-guided versus ultrasound-guided injections
This is one of the most common practical questions, and the literature still doesn't give a single best answer. Some clinicians are very comfortable using anatomy they can feel. Others prefer ultrasound to improve accuracy and visualize nearby structures.
From the patient side, the experience may not feel wildly different. What usually matters more is the skill and familiarity of the person doing the procedure, along with whether the technique matches your anatomy and clinical setting.
A few practical points can reduce stress before you go:
- Bring someone if you're anxious: Even if you end up feeling fine, support helps.
- Plan a lighter day if possible: You may want quiet time afterward, especially if your nervous system is already flared.
- Ask about aftercare before the injection starts: It's easier to remember instructions before, not after.
Some people drive home and return to normal activity shortly after. Others want a slow, low-stimulation rest of day. Both responses can be completely reasonable.
If you develop a sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury, seek immediate medical care. Those are red flags and should not be treated as routine migraine symptoms.
Risks Side Effects and Treatment Alternatives
You get the injection, head home, and then start asking the question that matters more than the procedure itself. Was this worth it for the amount of relief I might get?
That is the right lens for this section. A greater occipital nerve block can be very helpful for some people, but it also comes with trade-offs. The practical decision is not just about whether it can help. It is about how much relief you are hoping for, how long that relief might last, and what level of inconvenience or risk feels acceptable to you.
Common side effects versus more serious concerns
The common side effects are usually short-lived and centered around the injection area. People often describe soreness, tenderness, swelling, temporary numbness, dizziness, or an odd scalp sensation. If your scalp feels “off” for a while, that can be unsettling, especially if migraine already makes you hyper-aware of every sensation. In many cases, though, these effects fade on their own.
More serious problems are less common, but they are still worth asking about before you agree to the procedure. These include infection, bleeding, a temporary worsening of headache, or irritation from the injection itself. If your clinician uses a steroid along with the numbing medicine, repeated injections may carry added concerns such as local skin thinning or changes in the tissue near the injection site.
Technique also affects the trade-offs. One clinician may use anesthetic alone. Another may add steroid in hopes of longer relief for the right patient. One may prefer landmarks by touch, while another uses ultrasound. From a patient perspective, the practical question is simple: what does this specific approach add, and what extra downsides come with it?
A useful way to think about risk is this. A GON block is usually a low-risk procedure, but “low risk” does not mean “zero risk,” and it does not guarantee meaningful relief.
Where this fits among other migraine treatments
A greater occipital nerve block works best as part of a plan with a clear job description. For some people, that job is to calm a prolonged flare. For others, it is a short-term reset while waiting for a preventive treatment to start working. Some people try it because pain clusters around the back of the head or upper neck, which can make this option more appealing.
Other parts of migraine treatment can still matter just as much:
- Lifestyle support: regular sleep, meals, hydration, and reducing trigger pileup
- Acute treatment: medicine or other tools used during an attack
- Preventive treatment: treatment aimed at reducing how often attacks happen or how hard they hit
- Other procedures or devices: options that may fit better depending on your migraine pattern, anatomy, and medical history
Here is the simplest comparison:
| Option type | Best thought of as |
|---|---|
| GON block | A targeted procedure that may reduce pain signals for a limited period |
| Preventive treatment | A longer-term effort to lower migraine frequency or severity over time |
| Acute treatment | Something you use during an active attack |
| Tracking and pattern recognition | A way to see whether the treatment changed anything meaningful |
That last row matters more than it may seem in the moment. If relief lasts two days, two weeks, or not at all, that information helps shape what comes next. Using a migraine tracking app to monitor headache days, pain intensity, and response after treatment can make that pattern much easier to spot.
If you are choosing between options, skip the abstract question of which treatment is “best.” Ask a more grounded one instead. Which option fits the job you need done right now, and what trade-offs come with that choice?
Integrating a GON Block into Your Migraine Plan
The most useful thing you can do before a GON block is show up with a clear picture of your migraine pattern. The most useful thing you can do after one is track the response carefully enough that you and your clinician can tell whether it was worth repeating.
Questions to bring to your appointment
Good appointments are specific. If your clinician says a GON block is an option, these are the kinds of questions that can turn a vague idea into a real decision:
- Am I a good candidate based on my migraine pattern? Ask how your symptoms and pain location affect the decision.
- What do you use in the injection? This helps clarify whether the plan includes anesthetic alone or anesthetic plus steroid.
- How do you perform it? Ask whether they use landmarks by touch, ultrasound, or both in different cases.
- What would count as success for me? Relief can mean lower intensity, fewer attacks, shorter attacks, or even a break in a prolonged flare.
- What's the next step if it helps only briefly? This gets at repeat timing and whether the block is a bridge or part of a broader plan.

What to track after the procedure
Memory gets unreliable fast when you live with migraine. That's especially true if you're trying to decide whether a procedure helped “enough.”
Use a simple tracking system for at least these items:
- Attack frequency: Did attacks happen less often after the block?
- Pain severity: Were attacks milder, even if they still happened?
- Function: Could you work, read, drive, parent, or sleep more normally?
- Timing: How quickly did relief begin, and how long did it last?
- Side effects: Note soreness, dizziness, numbness, or anything unexpected.
A structured migraine tracking app that logs symptoms, timing, and patterns can make that much easier, especially if you're trying to compare before-and-after periods without relying on migraine-brain memory alone.
The goal isn't perfect note-taking. It's having enough evidence from your own life to answer one question honestly: did this meaningfully improve my month?
If you want an easier way to track migraine patterns before and after treatments like a GON block, Relief can help you log symptoms, triggers, and timing so you can spot what's changing.