
When your face tingles during a headache, it's hard not to think of the worst. The short answer is that headache facial tingling can happen with migraine, especially as a sensory aura, but sudden numbness or tingling with weakness, speech trouble, confusion, or vision changes needs immediate medical care.
That distinction matters because this symptom sits in an uncomfortable middle ground. Sometimes it's part of a familiar migraine pattern. Sometimes it's a warning sign you shouldn't try to explain away. This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Table of Contents
That Unsettling Feeling Headache and Facial Tingling
If you're reading this while touching your cheek, lip, or temple and wondering whether this is “just migraine,” your concern is reasonable. Facial tingling during a headache can be a migraine symptom, but the safety question depends on the pattern. Gradual, recurrent, familiar episodes are more reassuring. Sudden, dramatic, or clearly different episodes are not.
Migraine can cause tingling or numbness in the face and body before, during, or after an attack. At the same time, facial tingling can also appear with stroke, multiple sclerosis, trigeminal neuralgia, infection, anxiety, vitamin deficiencies, or nerve compression, as summarized by Healthgrades on tingling in the face.
Practical rule: Don't ask only “What does tingling mean?” Ask “How did it start, where is it, what came with it, and is this my usual pattern?”
That's the frame I use in clinic. Not every frightening symptom is dangerous, but the details matter. When you focus on timing, location, and associated symptoms, you give yourself and your doctor a much better chance of separating a migraine-related event from a neurologic emergency.
Understanding the Link Between Migraine and Facial Paresthesia
Migraine is a complex neurologic disorder, and sensory symptoms can be part of the attack. Facial tingling often fits that picture when it follows a pattern you recognize.
What paresthesia means
Paresthesia is the medical term for tingling, pins and needles, burning, or numbness. Giving the symptom a clinical name matters. It helps separate the feeling itself from the fear it creates, which makes it easier to describe clearly to a doctor.
In migraine, paresthesia often occurs as part of aura. Aura refers to temporary neurologic symptoms that can appear before the headache, during it, or sometimes with little head pain at all. Sensory aura may involve the cheek, lip, tongue, hand, or arm, often on one side. If you are still sorting out where these symptoms fit in the course of an attack, this explanation of migraine prodrome and the phases around an attack can help clarify the timeline.
Why migraine can cause it
The practical explanation is that migraine can temporarily disrupt how the brain handles sensory signals. In patient education reviewed by HealthCentral's article on tingling in the head, migraine-related sensory symptoms are described as transient and often one-sided. That fits what many patients report in clinic.
The more useful question is not, “Can migraine cause facial tingling?” It can. The better question is, “Does this tingling behave like my migraine usually behaves?”
That is where pattern recognition helps:
- Timing: Migraine-related tingling usually appears in a repeatable part of the attack, such as before the pain or early in the headache.
- Location: It often affects the same side or a similar path each time, such as cheek to lip or face to hand.
- Associated symptoms: Light sensitivity, nausea, visual aura, or a familiar throbbing headache make migraine more likely.
- Course: Symptoms that build, spread, and then fade are generally more consistent with aura than symptoms that strike all at once and stay fixed.
I pay close attention when a patient says, “It starts in my left lip, climbs into my cheek over 10 minutes, then the headache follows.” That history is more reassuring than, “Half my face went numb instantly, and this has never happened before.”
A few clinical realities are worth keeping in mind. Migraine-related tingling is often brief. A symptom can still deserve evaluation even when it is mild, if it is completely new or does not match prior attacks. Anxiety can make tingling feel louder and more threatening, but it does not mean the sensation is made up. Local problems such as dental disease, sinus irritation, or nerve compression usually follow a different pattern and do not line up neatly with migraine phases.
When facial tingling matches your usual migraine rhythm, it is often frightening but not automatically dangerous. First episodes are different. Those deserve more caution, especially when the timing, location, or companion symptoms break from your established pattern.
Is It Migraine Aura or Something More Serious
This is a common initial question. The hardest part is that tingling itself is not the deciding factor. The deciding factor is the overall pattern.
The pattern matters more than the sensation
A migraine sensory aura usually has a rhythm to it. It tends to be recurrent, often feels familiar once you've had it more than once, and may build in a more gradual way. More urgent neurologic causes tend to feel abrupt, new, and disruptive, especially when other deficits arrive at the same time.
Healthline's patient guidance puts the key distinction this way: migraine-related tingling is typically recurrent and develops gradually, while sudden unilateral facial numbness, especially with confusion, balance problems, or vision changes, requires immediate evaluation, as explained in Healthline's article on tingling in the face.
Another clue is where the symptom sits in the timeline of your migraine. Some people notice tingling before the pain phase. Others notice it during the attack or after the worst pain eases. If you're still learning your migraine phases, it may help to understand what prodrome means in migraine, because many people confuse prodrome, aura, the pain phase, and postdrome.
Migraine aura vs stroke symptoms
Use this table as a triage aid, not a diagnosis tool.
| Symptom Feature | Typical Migraine Aura | Potential Stroke Warning Sign |
|---|---|---|
| Onset | Often builds gradually and feels similar to prior episodes | Often sudden, abrupt, clearly different |
| Pattern over time | May spread or “march” across an area | May appear all at once |
| Recurrence | Often repeats in a recognizable way across attacks | New or first-time neurologic deficit is more concerning |
| Location | Can be one-sided and may match the side of head pain | One-sided symptoms can also occur, especially if paired with weakness or droop |
| Associated symptoms | May occur before, during, or after migraine headache | Confusion, speech trouble, balance problems, facial droop, weakness, major vision change |
| How reassuring it is | More reassuring if it's familiar and isolated | Less reassuring if sudden, severe, or combined with other deficits |
A common mistake is to focus only on whether the tingling is on one side. Migraine aura can absolutely be one-sided. Stroke symptoms can also be one-sided. One-sided does not settle the question. What settles it is the company the symptom keeps.
Here's a practical way to think through an episode:
- Did it come on gradually or all at once?
- Is this the same as your usual migraine pattern, or clearly different?
- Did it stay as tingling, or did weakness, speech trouble, confusion, or vision loss join in?
- Did a recognizable migraine attack follow, or are you dealing with a neurologic symptom that doesn't fit your usual pattern?
A familiar symptom in a familiar sequence is less alarming. A new neurologic symptom, especially if sudden, deserves urgent evaluation.
If you're ever stuck between “this could be migraine” and “this could be serious,” choose safety. Migraine can mimic other conditions. Other conditions can mimic migraine.
Red Flag Symptoms That Require Immediate Medical Care
If headache facial tingling happens with certain symptoms, this is not a “wait and see” situation. Seek emergency care now.
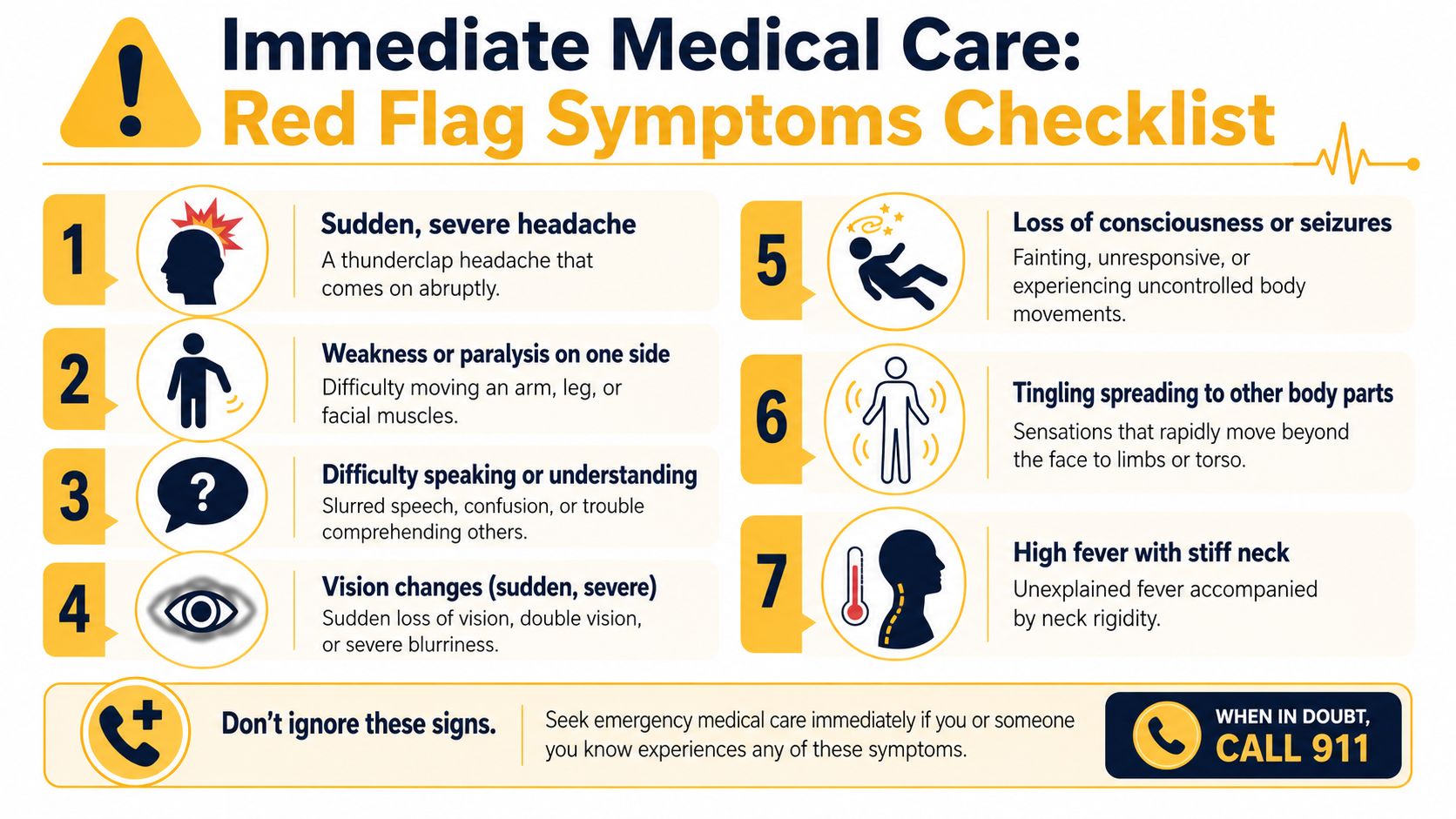
Go now if any of these happen
- Sudden one-sided weakness or paralysis. This includes trouble lifting an arm, moving a leg, or obvious facial droop.
- Slurred speech or trouble understanding language. If words won't come out right, don't drive yourself somewhere and hope it passes.
- Confusion or major change in alertness. Feeling “off” is different from being disoriented, hard to wake, or unable to follow conversation.
- Sudden vision changes. This includes loss of vision, severe blurring, or double vision.
- A sudden severe headache that feels explosive. Especially if it's unlike your usual attacks.
- Headache with fever and stiff neck. That combination needs prompt evaluation.
- Headache after head injury with neurologic symptoms. Don't assume it's your usual migraine.
Healthgrades notes that head tingling is often benign, but urgent evaluation is needed when it comes with one-sided weakness, paralysis, slurred speech, confusion, or vision changes, because these may signal stroke, multiple sclerosis, or another serious neurologic condition. If you're considering whether symptoms are severe enough for emergency care, this guide on when an ER migraine cocktail is used may help you think about what emergency teams are trying to rule out and treat.
This is not optional. If you have sudden neurologic changes, call emergency services or go to the nearest emergency department.
How a Doctor Diagnoses the Cause of Your Symptoms
The workup usually starts with a conversation, not a scan. That surprises many people, but the history often provides the clearest clue.
The history often gives the biggest clue
A clinician will usually ask about timing, frequency, duration, side, sequence, and associated symptoms. They want to know whether the tingling came before the headache, during it, or after it. They'll ask whether it always affects the same side, whether it spreads, how long it lasts, and whether you also had nausea, light sensitivity, sound sensitivity, or visual symptoms.
They'll also ask what makes this episode different from your baseline. If you have a long migraine history but suddenly describe a brand-new neurologic symptom, that changes the level of concern.
Bring details like these:
- Exact location. Cheek, lip, temple, jaw, scalp, tongue.
- Laterality. Left, right, both sides, or shifting.
- Sequence. Tingling first, then pain, or pain first, then tingling.
- Associated features. Speech changes, weakness, imbalance, visual symptoms, neck pain, fever.
- Recovery. Did it fully clear, partially improve, or linger?
What the exam and tests are looking for
The neurologic exam checks whether your nervous system is functioning normally right now. A clinician may test facial movement, sensation, strength, reflexes, coordination, eye movements, speech, and gait. They're trying to determine whether the symptom behaves like a transient migraine phenomenon or points toward a structural, vascular, infectious, or inflammatory problem.
Sometimes no imaging is needed, especially when the story fits a stable, established migraine pattern and the exam is normal. In other situations, a doctor may order a CT scan or MRI to rule out other causes. That's more likely when symptoms are new, the pattern has changed, the exam is abnormal, or red flags are present.
Bring a timeline, not just a label. “Left cheek tingling for 15 minutes, then right-sided head pain and light sensitivity” helps far more than “face numbness with headache.”
The goal isn't to prove that you're worried. The goal is to hand over the details that make good diagnosis possible.
Common Treatments and Management Strategies
Treatment works best when it matches the pattern.
If your episodes fit a familiar migraine pattern, management usually has three goals: reduce how often attacks happen, treat them early enough to limit escalation, and lower the disruption caused by tingling or numbness when it does occur. If the pattern does not fit migraine, the plan has to change. Facial tingling from a pinched nerve, vitamin deficiency, infection, anxiety, or another neurologic problem will not respond well to a migraine plan alone.
For migraine-related facial tingling, I usually frame treatment in two lanes: what you do between attacks, and what you do at the start of one. That distinction matters because a person with rare, predictable episodes needs a different strategy than someone with frequent attacks or lingering sensory symptoms.
If the tingling is part of migraine
Migraine is common enough that having a treatment plan matters. As noted earlier, this is not a rare problem, and many people do better once the plan is adjusted to the timing and character of their attacks.
A practical migraine plan often includes:
- Daily habits that lower attack frequency. Regular sleep, consistent meals, hydration, stress management, and avoiding personal triggers can reduce how often the brain shifts into a migraine state. This advice sounds simple. In practice, it often makes the difference between occasional attacks and a pattern that keeps recurring.
- Early treatment for the headache phase. Some people use nonprescription pain relievers. If you need them often, or if your symptoms have changed, it is time to review that with a clinician rather than keep guessing.
- Prescription acute medication. A doctor may recommend a medication to take when symptoms begin. Timing matters. A treatment that works well when taken early may work poorly once the attack is fully established.
- Preventive treatment. If attacks are frequent, disabling, prolonged, or difficult to control, preventive medication may be appropriate. The trade-off is straightforward. Prevention can reduce attack burden, but it also means taking a treatment regularly and monitoring for side effects.
Pattern recognition helps here too. Tingling that predictably builds, then gives way to headache and light sensitivity, is managed differently from tingling that appears out of nowhere, lasts much longer than usual, or starts happening without the rest of your typical migraine features.
One practical mistake is treating every episode as interchangeable. They are not. Some attacks are mostly pain. Some are mostly sensory. Some need early abortive treatment. Others signal that the overall migraine plan is no longer doing enough.
If the cause is something else
Once the pattern points away from migraine, treatment follows the diagnosis, not the symptom label. Reassurance is useful only when the story and exam support it. Imaging can help rule out dangerous causes, but it does not replace a careful history. The best treatment is the one that fits the mechanism causing the tingling.
That is why modest, concrete self-management tends to work better than vague advice. Reduce triggers you can control. Use the treatment plan you and your clinician agreed on. Reassess if the location, timing, duration, or associated symptoms change. If you want a structured way to keep that information straight, use a migraine log template that captures symptom timing and sequence.
Track Your Symptoms to Uncover Your Patterns
When a symptom can mean “familiar migraine aura” in one situation and “get checked urgently” in another, memory is not enough. Tracking gives you something more reliable than hindsight.
What to log every time
Individuals remember the pain. They don't remember the sequence. For headache facial tingling, the sequence is often the key.
Log these details each time:
- Start time and build-up. Did the tingling creep in or hit suddenly?
- Exact location. Left cheek, right lip, temple, scalp, jaw, tongue.
- Duration. Note when it fully resolved, not just when the headache took over.
- Headache relationship. Before, during, after, or without head pain.
- Associated symptoms. Light sensitivity, nausea, visual change, weakness, speech trouble, balance issues.
- Context. Sleep disruption, stress, weather change, missed meal, illness, alcohol, exertion.
If you want a structured way to do this, a simple migraine log template you can follow consistently can make your notes much more useful.
Why tracking changes the doctor visit
A good symptom log can shift an appointment from vague and frustrating to specific and productive. Instead of “sometimes my face tingles,” you can say, “It happens on the left, lasts briefly, and usually comes before the pain.” That gives your clinician a pattern to evaluate.
For people who prefer digital tracking, Relief is one tool that lets you log symptoms, medications, triggers, and environmental factors like weather, air quality, and pollen so recurring patterns are easier to spot over time.
A short demo makes that more concrete:
Tracking also helps you notice when a pattern is no longer your pattern. That's one of the most valuable safety benefits. You're not just collecting data. You're learning what is typical for you, which makes it easier to recognize when something is not.
The most useful migraine diary is the one you can keep during real life, not the perfect system you abandon after three days.
If you want a simple way to log tingling, headache timing, triggers, and changing patterns in one place, Relief can support tracking and awareness without replacing medical care.