Your worst migraine keeps showing up right before your period, or on day one, and by now it doesn't feel random at all. That pattern matters. Hormonal migraine prevention is possible, especially when you stop treating each attack like a surprise and start building a plan around your cycle.
For many people, the hardest part isn't just the pain. It's the repetition. You arrange your week, protect your sleep, drink water, avoid obvious triggers, and the attack still lands on schedule. That can make migraine feel less like a health condition and more like an appointment you never agreed to keep.
The good news is that predictability gives you something useful. A migraine that follows a hormonal pattern can often be approached more strategically than one that seems to come out of nowhere. You and your doctor can use timing, symptoms, and cycle data to decide whether hormonal options, short-term prevention around your period, daily preventives, or lifestyle adjustments make the most sense for you.
Table of Contents
Introduction
If your migraine attacks arrive like clockwork around your period, you're not imagining it and you're not overreacting. A cyclical pattern is one of the clearest clues in migraine care, because it tells you where prevention may work best.
Hormonal migraine prevention works best when you think in phases, not isolated attacks. Instead of asking only, “What should I take when the migraine starts?” it helps to ask, “What tends to happen in my body this week, and how can I lower my risk before the attack begins?”
That shift changes everything. Some people do best with continuous hormonal strategies that reduce abrupt hormone changes. Others need short-term prevention only during the days when their risk rises. Many also need a simpler layer underneath all of that: steadier sleep, fewer skipped meals, lower stress load, and better tracking.
Practical rule: If your attacks are predictable, your prevention plan should be predictable too.
A good plan doesn't have to be complicated. It does need to be personal. Your cycle may be regular or irregular. You may have migraine with aura, without aura, or several attack types. You may be dealing with perimenopause, contraception decisions, or attacks that used to be occasional and are now more disruptive.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
What Exactly Is a Hormonal Migraine
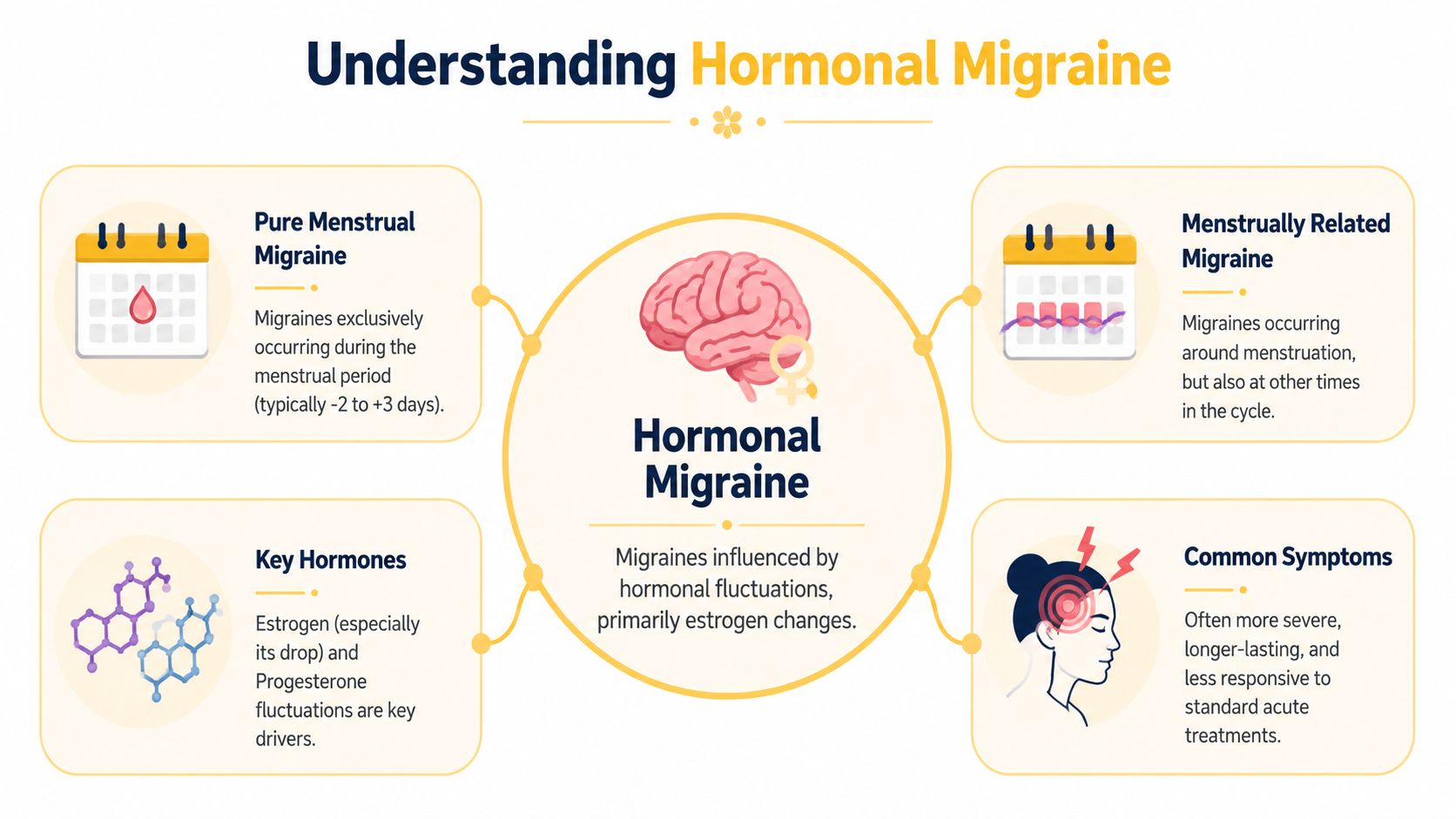
A hormonal migraine is a migraine attack linked to hormone fluctuations, especially changes in estrogen. For many people, the trigger isn't “having low estrogen” all month. It's the drop in estrogen that happens at a specific point in the cycle.
How the cycle affects the brain
Think of estrogen like a tide. When the water moves gradually, the shoreline adjusts. When the tide pulls out quickly, what's exposed becomes more vulnerable. In menstrual migraine, that hormone withdrawal appears to lower the brain's resistance to migraine triggers.
That's why timing matters so much. Menstrual migraine affects about 20% to 25% of women with migraine, and attacks often happen in the two days before a period and the first three days of flow, right when estrogen drops significantly, according to clinical guidance on managing menstrual migraine from the Association of Migraine Disorders.
This is also why hormonal migraine prevention is usually designed to smooth that drop, or to protect you during that high-risk window, rather than trying to raise hormone levels in a vague way.
Two patterns that matter
Doctors often think about menstrual migraine in two broad patterns:
PatternWhat it meansWhy it mattersPure menstrual migraineAttacks occur only around the menstrual windowPrevention can often focus tightly on that short time frameMenstrually related migraineAttacks happen around menstruation and at other times tooYou may need both cycle-based prevention and a broader migraine plan
If you're not sure which pattern fits you, tracking usually answers that question better than memory does. People often remember the worst attacks, but not the exact timing.
A lot of readers also wonder whether hormonal migraine is “just a bad period headache.” It isn't. Migraine is a neurological condition. It can come with nausea, sensitivity to light or sound, aura, dizziness, and exhaustion, not just head pain.
If you're trying to sort out your broader trigger profile, it can help to review common migraine risk factors and how they interact. Hormones may be the main driver, but they rarely act alone.
A hormone-linked migraine pattern is frustrating, but it also gives you a usable map.
Medical Prevention Strategies to Discuss With Your Doctor
When hormonal migraine prevention works well, it's usually because the strategy matches the pattern. A person with tightly predictable attacks before each period may need a different approach from someone with migraine throughout the month that becomes worse around menstruation.

Hormonal treatments
The main hormonal idea is straightforward. If estrogen withdrawal is the trigger, then reducing that withdrawal may reduce attacks.
For people with migraine without aura, continuous combined hormonal contraception can be an effective preventive option because it minimizes the hormone-free interval and helps stabilize estrogen exposure, as described by the American Migraine Foundation on menstrual migraine treatment and prevention. In practice, that can mean using combined hormonal methods without the usual placebo break, or with a shortened break, if a clinician decides it's appropriate.
That said, hormonal options are not interchangeable. Some people improve on them. Others don't. Some can't use estrogen-containing methods safely at all.
Targeted perimenstrual prevention
If your attacks are highly predictable, your doctor may suggest short-term prevention only around your menstrual window. This is often called mini-prophylaxis or perimenstrual prevention.
The timing can be quite precise. For predictable menstrual migraine, mini-prophylaxis often starts 2 to 3 days before expected menses. Regimens identified in review include frovatriptan 2.5 mg twice daily or naproxen 550 mg twice daily, taken for about a week, as effective options during the high-risk window, according to this review of menstrual migraine management in Human Pharmacology and Physiology.
That doesn't mean those options are right for everyone. It does show the logic of this approach. You don't necessarily need to medicate the entire month if your risk is concentrated in a very narrow slice of it.
Some clinicians may also discuss estrogen supplementation during the menstrual week for carefully selected patients. The point is still the same: blunt the withdrawal trigger.
Short-term prevention makes the most sense when your cycle is predictable enough to let you get ahead of the attack.
General daily preventives
If you have migraine throughout the month, or if menstrual attacks are only one part of a larger pattern, cycle-based prevention may not be enough on its own. In that situation, a doctor may recommend a general daily preventive plan and then layer menstrual-specific strategies on top.
This is often where real-world care becomes more nuanced than online lists. A person may need one plan for background migraine frequency and a second plan for the menstrual spike. That combination approach is common in practice.
A few trade-offs are worth keeping in mind:
- Predictable cycles favor timing-based prevention. If your period arrives regularly, mini-prevention may be easier to use well.
- Irregular cycles complicate short-term strategies. When timing shifts, you may need broader preventive support.
- Migraine with aura changes the conversation. Estrogen-containing options require extra caution.
- Other vascular risk factors matter. Your doctor should assess the whole picture, not just migraine timing.
Lifestyle and Non-Medical Prevention Approaches
Lifestyle work can sound underwhelming when you're dealing with a disabling neurological condition. But during hormonally vulnerable days, the threshold for an attack may be lower. That means the ordinary stressors you can usually absorb may hit harder.
Why lifestyle matters more during hormonal shifts
When estrogen is falling, your system may be less forgiving. A missed meal, poor sleep, dehydration, or a stressful day at work can carry more weight than it would in another part of the month.
That doesn't mean lifestyle changes cure hormonal migraine. They don't. It means they can help raise your baseline resilience so the hormonal trigger has less force.
Three areas commonly matter most:
- Sleep consistency: Go to bed and wake up on a stable schedule, including weekends if you can.
- Food and hydration: Avoid long gaps without eating, and keep fluids steady rather than trying to “catch up” late.
- Stress load: You may not be able to reduce stress completely, but you can reduce how chaotic your nervous system feels.
What to tighten up before your high-risk days
The luteal and menstrual parts of the cycle are often where people benefit from being more deliberate. This is usually the wrong time to experiment with all-nighters, skipped lunches, or hard training if those tend to trigger attacks for you.
A practical reset often looks like this:
- Plan meals earlier: Put easy food in reach before the busy week starts.
- Protect bedtime: Don't save sleep hygiene for after the migraine begins.
- Lower stimulation: Build in quieter evenings if light, sound, or sensory overload tends to stack on top of hormonal triggers.
- Use gentle movement: Walking, stretching, or other light activity may be more realistic than pushing through intense workouts.
- Discuss supplements carefully: Magnesium has data-supported use in menstrual migraine prevention when used in a cycle-based way, but it's still worth reviewing with your clinician first.
If food patterns seem to be part of the picture, a structured approach to building a migraine-friendly eating routine can help you separate real triggers from guesswork.
The goal isn't a perfect lifestyle. It's fewer avoidable hits during the days your brain is already more vulnerable.
How to Create Your Personal Prevention Plan
A personalized plan works better when it follows the rhythm of your cycle instead of treating every day the same. You don't need to do everything at once. You need to know when to emphasize which tools.
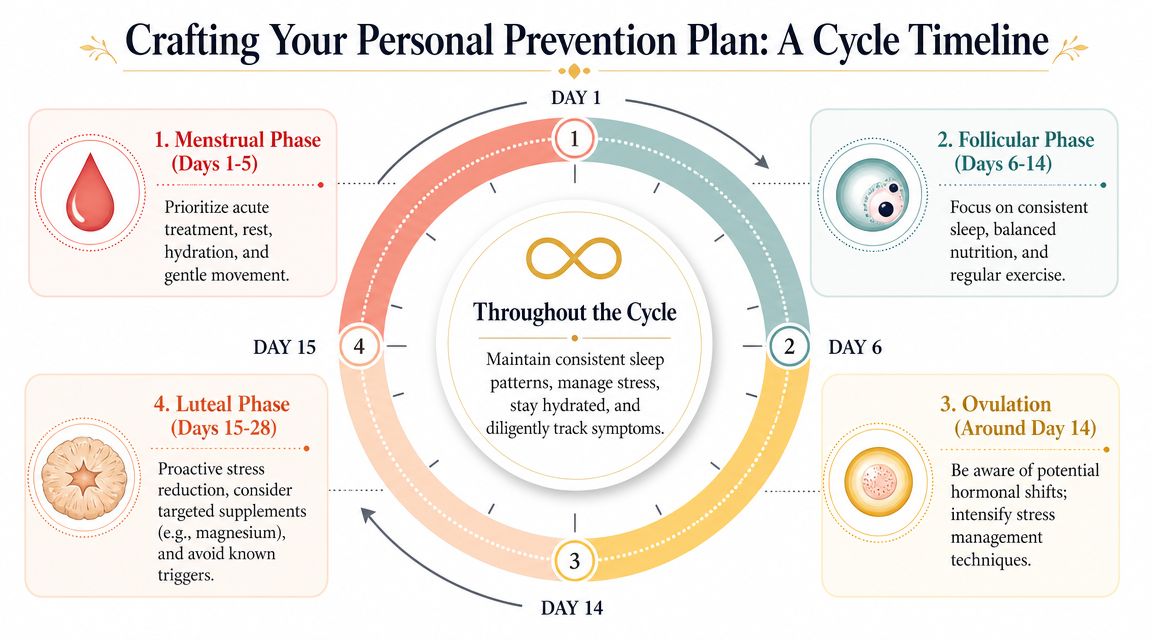
Follicular phase
After your period ends, many people enter a more stable stretch. This is often the best time to focus on consistency rather than crisis management.
Use this phase to build the basics that make the rest of the month easier:
- Set your routine: Regular sleep, regular meals, regular hydration.
- Review the last cycle: What day did symptoms start? What helped? What felt useless?
- Refill and prepare: Make sure anything you use for acute treatment or prevention is available before your risk window opens.
If you tend to forget details once the migraine passes, this is the time to write them down.
Later in the cycle, it helps to revisit the timing visually:
Ovulation and luteal phase
Not everyone notices symptoms around ovulation, but some do. The bigger practical issue for many people is the luteal phase, when the next hormone drop is approaching.
This is the phase where prevention often becomes more active. If you and your doctor are using a perimenstrual strategy, this is when you'll want your timing plan clear. If your main tools are non-medical, this is the week to become more protective of sleep, meals, hydration, and sensory load.
A useful checklist for this phase:
- Check your calendar: Estimate when your high-risk days are likely to begin.
- Reduce stackable triggers: Long workdays, skipped meals, alcohol, and sleep loss can combine badly here.
- Simplify commitments: If possible, avoid loading the highest-demand tasks into the days you usually feel most fragile.
- Watch for early signals: Prodrome can include fatigue, food cravings, mood shifts, neck pain, or brain fog before head pain starts.
Menstrual phase
This is the part of the cycle where your prevention plan becomes most concrete. If your migraines are tied closely to menstruation, this is usually the window where targeted prevention or your clinician-approved acute plan matters most.
During these days, keep your approach simple and repeatable:
PhaseMain focusPractical emphasisDays leading up to bleedingAnticipate riskStart the plan you and your doctor choseFirst days of flowReduce escalationRest, hydrate, eat regularly, treat early if advisedRecovery after attackLimit the rebound effectResume routine gently, note what happened
Don't judge the plan by one cycle alone. Hormonal migraine prevention often becomes clearer over several cycles, especially when tracking is part of it.
The Power of Tracking and When to See a Doctor
Without tracking, hormonal migraine prevention is mostly guesswork. With tracking, patterns become visible enough to act on.
What to track each month
You do not need a perfect diary. You need a useful one. The key is to log enough information to connect your migraine pattern to your cycle and to see whether a prevention strategy is helping.
Track these basics:
- Cycle timing: First day of bleeding, expected next period, and any irregularity.
- Migraine timing: Start time, end time, and how it lined up with your cycle.
- Symptoms: Aura, nausea, photophobia, phonophobia, dizziness, neck pain, fatigue, postdrome.
- Severity and function: Could you work, drive, exercise, or concentrate?
- What you used: Any acute medication, preventive step, or self-care measure.
- Possible co-triggers: Poor sleep, missed meals, travel, stress, weather shifts, or illness.
Tracking also helps answer a question that matters clinically: is the migraine menstrual, mostly menstrual, or only one part of a broader migraine pattern?
If you want a digital system instead of paper notes, a dedicated migraine tracking app that helps you spot patterns can make this much easier.
When to seek medical help
If you suspect a hormonal pattern, it's worth bringing that observation to a healthcare professional. Don't wait until the attacks become impossible to manage.
Ask for medical review if:
- Your attacks cluster around menstruation
- Your current acute treatment isn't working well
- You want to discuss hormonal migraine prevention
- You have migraine with aura
- Your pattern has changed recently
- You're in perimenopause or dealing with cycle irregularity and worsening migraine
The need for supervision is especially important with hormonal options. Caution around hormonal prevention comes from historical data linking some estrogen-containing contraceptives to increased ischemic stroke risk, especially in people with migraine with aura. Modern guidance, including WHO classifications, distinguishes between hormonal options and supports individualized risk assessment with a doctor, as reviewed in this PubMed Central article on hormonal contraception and migraine.
Seek immediate medical care for a sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury.
Those symptoms need urgent evaluation. They should not be managed as a routine hormonal migraine.
Taking the First Step Toward Fewer Migraine Days
Hormonal migraine can feel relentless because it keeps returning on a schedule that seems stronger than your plans. But that schedule is also the opening. A pattern you can recognize is a pattern you can prepare for.
The most effective hormonal migraine prevention usually isn't one magic fix. It's a plan built around your real cycle, your real symptoms, and your real risks. For some people that means hormonal treatment. For others it means short-term prevention around menstruation. For many, the strongest approach combines medical care, lifestyle support, and better timing.
If you're not sure where to start, start with observation. Log your cycle. Log your symptoms. Mark when the earliest warning signs appear. Bring that record to your doctor and ask for a prevention plan that fits the rhythm of your month, not a generic template.
You deserve more than reacting late every time. You deserve a strategy.
By tracking your cycle, symptoms, and likely triggers in one place, Relief can help you spot patterns earlier and bring clearer information into conversations with your doctor.