
Triptans work by targeting serotonin receptors in the brain to constrict swollen blood vessels and block pain signals, effectively stopping a migraine attack in its tracks. They can reduce migraine symptoms or abort attacks within 30 to 90 minutes in 70–80% of patients according to this triptan overview.
You probably know the moment. The light starts to feel wrong. Your neck tightens. Maybe your stomach turns, or words get harder to find. You're standing there asking yourself the same question you've asked before. Should I take my migraine medicine now, or wait and see if this gets worse?
That question matters more than is often recognized. Triptans are not generic pain relievers. They're migraine-specific drugs that act on the trigeminal system, the blood vessels around the brain, and pain-processing pathways in the brainstem. That's why understanding the mechanism of action of triptans can make your treatment choices feel less like guesswork.
Migraine is also not the same thing as a regular headache. A migraine attack can include prodrome (early warning symptoms before pain), aura (temporary neurological symptoms such as visual changes), headache pain, and postdrome (the drained, foggy phase after the main attack). If you're still learning those phases, this guide to what prodrome means in migraine can help.

This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance. If you have a sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury, seek immediate medical care.
Table of Contents
- The practical difference between migraine treatment and headache treatment
- What readers usually get wrong
- They narrow pain-sensitive blood vessels
- They calm irritated trigeminal nerve endings
- They turn down pain transmission in the brainstem
That Familiar Feeling When a Migraine Attack Begins
A migraine attack often starts with uncertainty. You may notice photophobia (light sensitivity), phonophobia (sound sensitivity), nausea, yawning, food cravings, or a strange sense that something is off before the pain fully arrives. Then the debate starts. Is this really a migraine attack, or just a bad headache?
That's where triptans can feel confusing. People often hear that triptans “shrink blood vessels,” and that's not wrong, but it's incomplete. They also act on nerve endings involved in migraine and on pain pathways in the brainstem. That fuller picture matters, because it explains why triptans can stop an attack better than a standard painkiller for many people.
The practical difference between migraine treatment and headache treatment
A tension headache usually doesn't involve the same migraine-specific nerve pathways. Migraine does. That's why a migraine-specific medicine can behave very differently from ibuprofen or acetaminophen, even if the pain feels similar at first.
Many people don't need more willpower or a higher pain tolerance. They need treatment that matches migraine biology.
If you've ever thought, “Why did my medicine help one attack but not another?” the answer often lives in timing, migraine phase, and how far the attack has progressed before treatment starts.
What readers usually get wrong
Two ideas trip people up most:
- “If it's pain medicine, later should be fine.” Triptans aren't best understood as simple pain blockers. They work best when they interrupt migraine processes early.
- “If my blood pressure is normal, blood vessels can't be part of this.” Migraine isn't just a blood vessel problem. It involves nerves, inflammatory signaling, and central pain processing.
- “If I have aura, I should take it the second aura starts.” That's not the usual recommendation for triptans, which is covered later in this article.
A good mental model is this: a triptan is less like a blanket painkiller and more like an emergency brake aimed at a specific migraine system. If you pull that brake before the whole train is speeding, you have a better shot at stopping the attack cleanly.
The Three-Part Action How Triptans Stop a Migraine
The mechanism of action of triptans makes more sense when you stop thinking about them as doing one thing. They act at 5-HT1B and 5-HT1D serotonin receptors and work through three connected pathways. According to NCBI Bookshelf on triptans, triptans exert their antimigraine effect through three distinct mechanisms: direct vasoconstriction of dilated intracranial vessels (via 5-HT1B receptors), inhibition of vasoactive neuropeptide release from trigeminal nerve terminals (via 5-HT1D receptors), and central inhibition of pain transmission in the brainstem's trigeminocervical complex.
A visual can make that easier to hold in your head.

They narrow pain-sensitive blood vessels
One part of migraine involves dilation of certain intracranial blood vessels. Triptans stimulate 5-HT1B receptors on vascular smooth muscle, which causes those vessels to constrict.
Consider it akin to a hose that has become overly widened and pressurized in the wrong place. Narrowing it back toward normal can reduce part of the painful signaling around the attack. This aspect is often highlighted initially.
But this is only one piece.
They calm irritated trigeminal nerve endings
Migraine also involves the trigeminal nerve, which helps carry pain information from structures in the head. During an attack, trigeminal nerve endings can release inflammatory neuropeptides such as CGRP and substance P. Those chemicals help amplify pain and neurogenic inflammation.
Triptans act at 5-HT1D receptors on those nerve endings and reduce that release. A useful way to picture it is a fire alarm system that has started blasting signals everywhere. Triptans don't just cover your ears. They help interrupt the alarm at the wiring.
Practical rule: Triptans work upstream in the migraine process. That's one reason they can feel very different from a standard over-the-counter pain reliever.
After this explanation, it's worth seeing a second format of the same idea.
They turn down pain transmission in the brainstem
The third action happens centrally, within the trigeminocervical complex in the brainstem, a region where incoming migraine pain signals get relayed and amplified. Triptans help inhibit nociceptive, meaning pain-related, neurotransmission there.
That means they aren't only working at the surface level of blood vessels or peripheral nerves. They're also helping reduce how strongly pain messages are passed along inside the central nervous system.
Here's the simplest way to remember the three-part model:
| Part of the process | What triptans do | Why it matters to you |
|---|---|---|
| Blood vessels | Constrict dilated intracranial vessels | Can reduce one source of migraine pain |
| Trigeminal nerve endings | Decrease release of CGRP and substance P | Helps limit inflammatory signaling |
| Brainstem pain pathways | Inhibit pain transmission centrally | May stop the attack from escalating |
That's why triptans are migraine-specific. They don't just dull pain. They target several parts of the migraine circuit at once.
Why Timing Is Everything for Triptan Efficacy
The advice to “take a triptan early” can sound repetitive until you know what's happening biologically. The key idea is central sensitization. That means the migraine pain system becomes more reactive and harder to quiet down once the attack has built momentum.
In plain language, your nervous system can move from “this attack is starting” to “everything is too loud, too bright, too painful, and even normal sensation feels amplified.” Triptans are much better at stopping that progression than undoing it after the system is already fully wound up.
Early treatment helps stop the cascade
The primary goal is not just pain relief. It's interruption of the migraine cascade before it becomes self-sustaining. Triptans are especially useful when they get in early enough to reduce inflammatory signaling and dampen pain transmission before central sensitization takes hold.
That's why timing changes outcomes. Clinical guidance summarized in The Migraine Trust's triptan guide says triptans are recommended as soon as possible after the onset of pain rather than during the prodrome or aura phase, and for migraine with aura, efficacy is maximized after the aura ends and pain begins, with a maximum of two doses per 24 hours.
A practical way to use that information is to notice your personal “pain starts now” moment. For some people that's the first true throb. For others it's the point when light sensitivity and one-sided head pain clearly line up in a familiar pattern.
Aura changes the timing
If you have migraine with aura, the timing can feel especially confusing. Aura can include flashing lights, zigzag lines, blind spots, numbness, or language difficulty before headache pain starts. The common recommendation for triptans is not to take them during aura, but after aura has finished and the pain phase begins.
That distinction matters because migraine phases are biologically different. A treatment that works best during the pain phase won't necessarily work best in the pre-pain phase.
Treating early doesn't mean treating at any unusual sensation. It means recognizing the beginning of your usual migraine pain pattern and acting promptly within the plan your clinician has given you.
If your attacks change shape, come on unusually fast, or stop responding to your usual plan, that's a good reason to check in with a healthcare provider rather than taking more medication.
Triptans in the Real World What to Expect
You feel the attack starting, you take the medication, and then the waiting begins. What you usually want to know next is simple. How quickly should this help, and what should you make of it if it no longer works the way it once did?
The answer starts with a practical detail. Triptans do not all arrive at the same speed. A tablet has to move through the stomach and be absorbed. A nasal spray can bypass some of that delay. An injection reaches the bloodstream faster. That difference matters during migraine because nausea, slowed stomach emptying, and a rapidly escalating attack can all interfere with how much medicine gets where it needs to go.
How fast they may work
Some people notice relief within the first part of an hour, especially with faster formulations and attacks treated before symptoms build too far. Others feel a more gradual change. Pain may ease first, then light sensitivity, nausea, or the foggy “I can't function” feeling.
That pattern can be confusing if you expect a single dramatic switch from migraine to normal.
A better way to judge response is to watch for signs that the attack is losing momentum. Can you open your eyes more comfortably? Can you think in full sentences again? Can you get through a basic task without every sound feeling sharp? Those changes count because triptans are trying to interrupt the attack process, not just erase head pain on a stopwatch.
A simple checklist helps:
- Look for pattern across several attacks. One unusually stubborn migraine can make a useful treatment look ineffective.
- Track function as well as pain. Relief includes being able to read, talk, work, rest, or tolerate light.
- Write down associated symptoms. Nausea, sound sensitivity, and light sensitivity often improve alongside pain.
- Note the formulation. A pill, nasal spray, and injection can feel very different in day-to-day use.
Why a triptan may seem less effective over time
If a triptan used to feel dependable and now feels hit-or-miss, timing is one possible reason. Small delays matter. Once a migraine has had more time to recruit pain pathways in the brain and brainstem, the attack can become harder to shut down. This connects back to the biology discussed earlier. The longer the process runs, the more likely central sensitization is to join in, and that often means a rescue medicine feels weaker even if the drug itself has not changed.
Other factors can also change the experience. Your attacks may be becoming more severe. Nausea or vomiting may be limiting absorption of an oral dose. You may be using the medicine more often because your migraine pattern has shifted, which is a clue that the larger treatment plan may need attention.
If your triptan seems less reliable than it used to, bring a log of attack timing, dose timing, formulation, and symptoms to your appointment. Those details often explain more than memory alone.
Medication overuse headache can complicate the picture in people with frequent attacks. The takeaway is awareness. If your rescue medication is starting to feel like a routine part of the week rather than an occasional tool, it is time to talk with your clinician about prevention, attack frequency, and whether your current plan still fits your migraine pattern.
Understanding the Safety Profile of Triptans
A triptan can feel almost routine right up until you read the warning label and see words about blood vessels, chest symptoms, or drug interactions. That contrast is unsettling. The safety profile makes more sense once you connect it to the same mechanism that makes these medicines useful during a migraine attack.
Why side effects happen
Triptans act on serotonin receptors involved in migraine signaling. Part of that action also narrows certain blood vessels. For many people, that effect is tolerated well. For someone with a history of coronary artery disease, prior stroke, uncontrolled high blood pressure, or other vascular disease, the same effect can change the risk calculation. The question is not whether triptans are "good" or "bad." The question is whether their mechanism fits your body and medical history.
That same receptor activity also explains some of the odd sensations people report after a dose. Tingling, warmth, flushing, pressure, heaviness, or chest tightness can happen. These symptoms are often brief and not dangerous, but they can feel dramatic if no one warned you first.
A useful comparison is a fire alarm versus a house fire. Some post-dose sensations are more like the alarm. They get your attention, but they do not automatically mean damage is happening. Severe chest pain, fainting, or symptoms that feel clearly different from your usual pattern need urgent evaluation because they may signal something more serious.
A practical safety check before and during use
A few habits make triptan use safer and less stressful:
- Review your cardiovascular history with your clinician. Past heart disease, stroke, peripheral vascular disease, and uncontrolled blood pressure matter because they relate directly to the drug's vessel-narrowing effect.
- Tell your clinician and pharmacist about every medicine and supplement you take. That includes antidepressants, anti-nausea medicines, and over-the-counter products. The goal is to catch interaction risks before you are treating an attack while in pain.
- Learn your own expected side effects. If warmth or tingling happens every time you use the same triptan and your clinician has already reviewed it, that pattern is less alarming than a brand-new symptom.
- Use the prescription exactly as written. Taking extra doses or combining acute treatments on your own can muddy the picture and increase risk.
One more point causes a lot of confusion. People often hear about serotonin syndrome and assume any serotonin-related medicine combination is automatically dangerous. The core message is simpler. Keep your medication list updated and let a clinician or pharmacist review it. If you want a patient-friendly example of how a newer non-triptan option differs, this guide to Nurtec side effects and weight changes gives helpful context.
When to get medical help
Get urgent care for severe chest pain, fainting, major neurological changes, shortness of breath, or symptoms that are clearly outside your usual migraine pattern.
Get prompt medical advice, even if it does not feel like an emergency, if side effects are repeating, worsening, or making you avoid treatment. A triptan only helps when you can use it with confidence. If fear of side effects is delaying treatment, that becomes a migraine management problem too.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance. If you have a sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury, seek immediate medical care.
The Next Generation Triptans vs Gepants and Ditans
If triptans are migraine-specific, why are there newer options? Mostly because migraine biology is complex, and not everyone can take or tolerate a medicine that constricts blood vessels.
That's where gepants and ditans come in. They're also prescription treatments for acute migraine, but they target different pathways.
How the targets differ
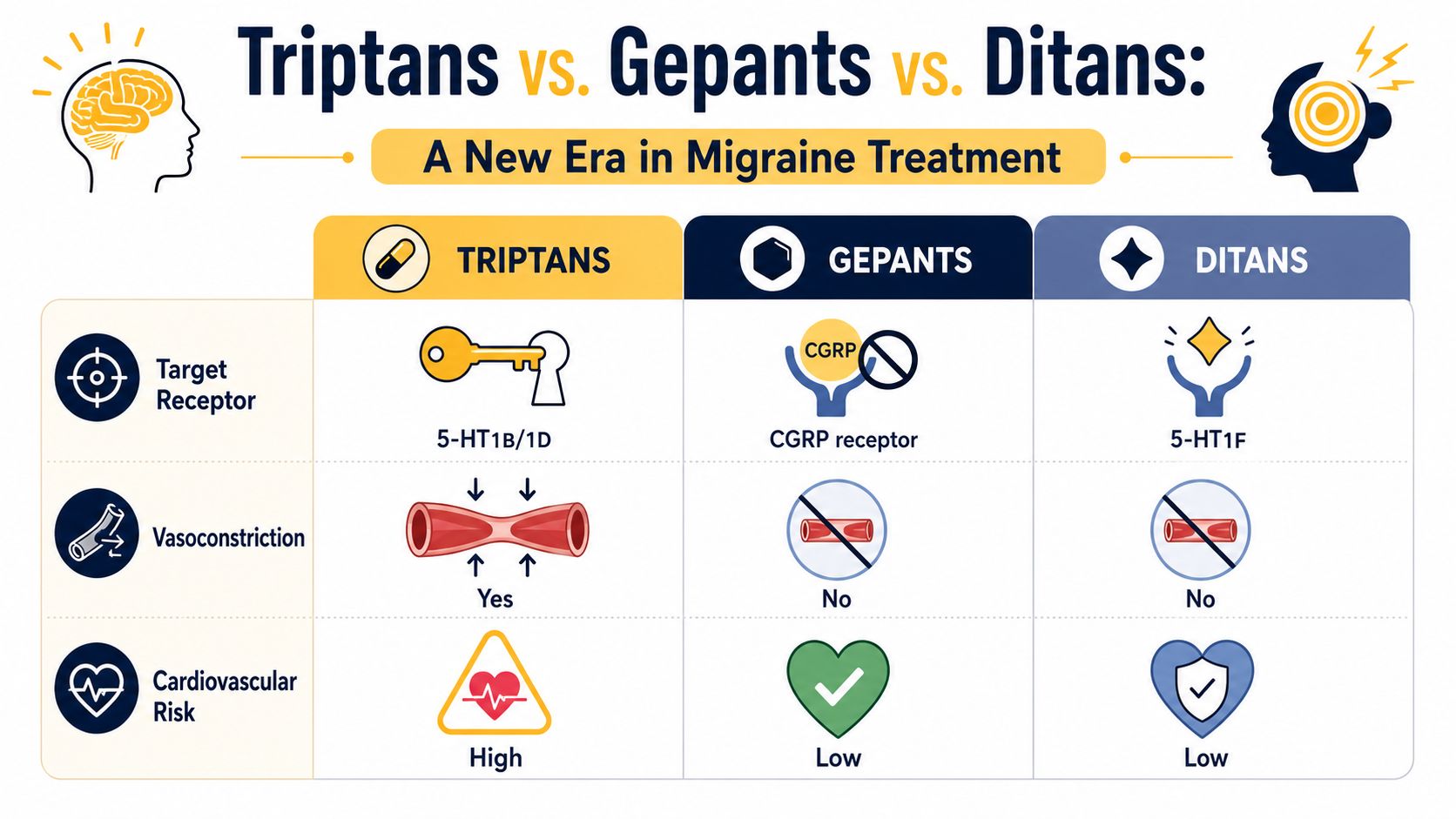
Triptans act mainly at 5-HT1B/1D serotonin receptors. Gepants block the CGRP receptor. Ditans target 5-HT1F receptors. That may sound technical, but the practical distinction is straightforward: these classes interrupt migraine signaling in different ways.
If you want a patient-friendly overview of one newer option, this article on Nurtec side effects and weight changes helps explain how CGRP-targeting treatment differs from older migraine drugs.
Why that difference matters
The biggest real-world difference is vascular effect. Triptans do cause vasoconstriction. Gepants and ditans generally do not. That's why newer classes may be options for some people who can't use triptans because of cardiovascular concerns.
Here's a simple comparison:
| Medication class | Main target | Vasoconstriction | Why a clinician may consider it |
|---|---|---|---|
| Triptans | 5-HT1B/1D | Yes | Acute migraine treatment when appropriate |
| Gepants | CGRP receptor | No | May be considered when vascular effects are a concern |
| Ditans | 5-HT1F | No | Another acute option with a different receptor target |
None of this makes triptans outdated. It just means there are now more ways to target migraine biology. If triptans don't work well for you, stop working reliably, or aren't safe in your situation, that's worth discussing with a qualified clinician.
Taking Control with Knowledge and Tracking
Once you understand the mechanism of action of triptans, the usual advice starts making more sense. Triptans work best when they interrupt migraine biology early, before the pain system becomes more sensitized and harder to calm down. That's the “why” behind taking them promptly when your migraine pain starts, rather than waiting to see if the attack becomes unbearable.
That knowledge can make you more confident, but it can also make you more observant. Notice when pain begins, whether aura comes first, how fast symptoms escalate, whether nausea changes absorption, and whether a medicine's effect is shifting over time.
A simple record can make those patterns visible. This migraine log template is a useful place to start if you want a clearer picture to share with your healthcare provider.
The goal isn't to become your own neurologist. It's to become a better witness to your own migraine pattern, so treatment decisions rely on evidence from your real life, not foggy memory after a hard attack.
Relief can help you track attack timing, symptoms, triggers, and medication response in one place, so you can spot patterns earlier and bring clearer information into conversations with your healthcare provider.