You are intimately familiar with your migraine patterns. So when a headache feels unusually intense, different, or frighteningly sudden, it's natural to wonder, is this a migraine or an aneurysm? The shortest answer is this: migraine pain usually builds, while a ruptured aneurysm typically hits all at once, reaching maximum intensity in less than a minute. That difference matters.
If you're reading this during a bad attack, take a breath and focus on one question first: Did this pain explode suddenly, or did it ramp up the way your migraines usually do? That won't diagnose you, but it gives you an immediate safety framework. This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
| Feature | Migraine | Ruptured aneurysm |
|---|---|---|
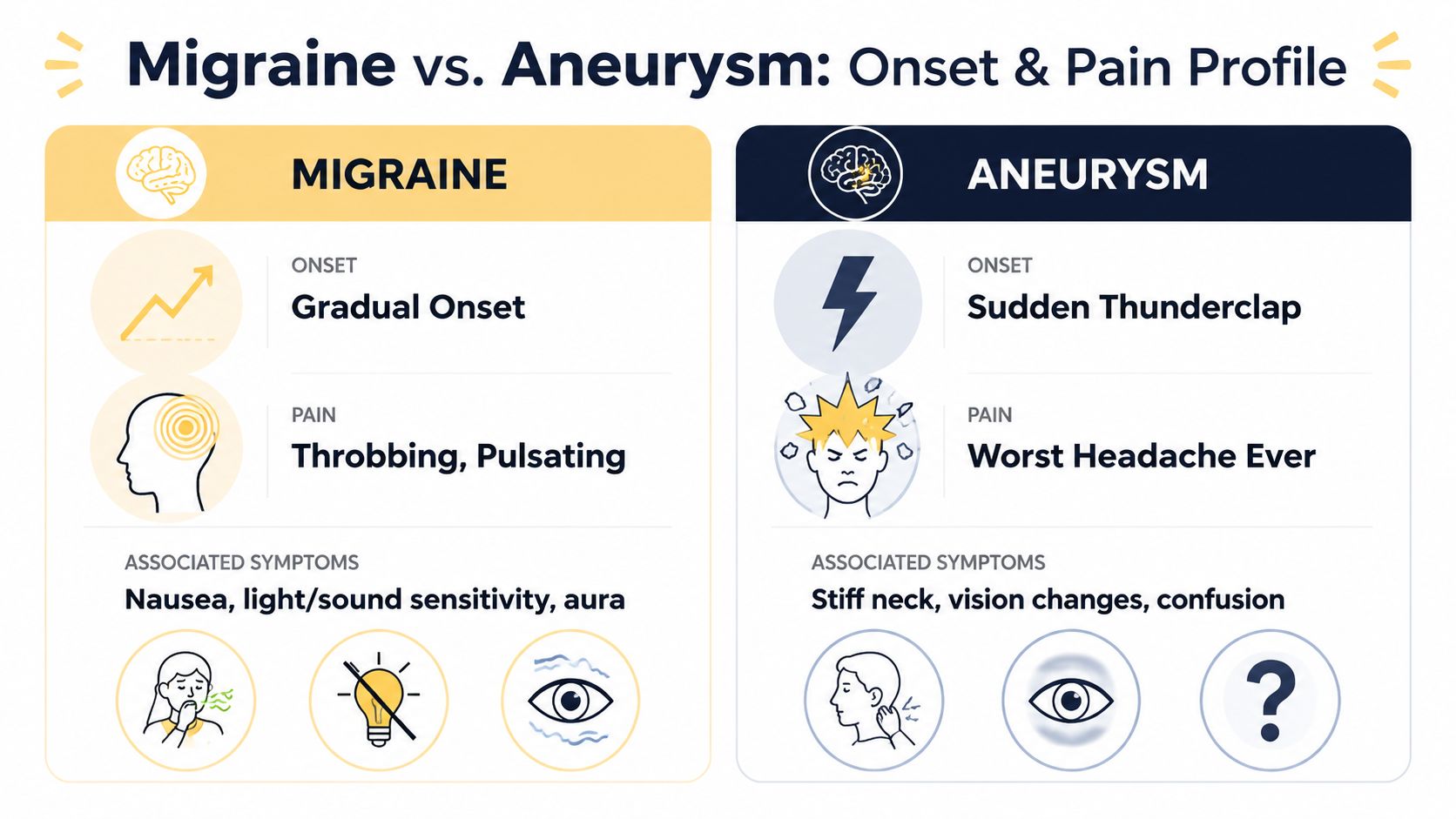
| How it starts | Usually builds gradually | Usually starts suddenly and peaks almost immediately |
| Pain pattern | Often throbbing or pulsating, commonly one-sided | Often explosive, severe, and not clearly one-sided |
| Typical timeline | Often unfolds in phases | Medical emergency, abrupt onset |
| Common associated symptoms | Nausea, light sensitivity, sound sensitivity, sometimes aura | Stiff neck, confusion, seizure, loss of consciousness, focal neurological symptoms |
| Response to usual migraine meds | May improve | Doesn't behave like a typical migraine attack |
| What to do | Use your usual plan and monitor symptoms | Seek emergency care right away |
Table of Contents
Is This a Migraine or Something More Serious
A common scene goes like this: you've had migraines for years, maybe even enough that other people downplay them. Then one day the pain feels stronger, stranger, or sharper than usual, and your brain jumps straight to the worst possibility. That fear is understandable.
The most important difference in a migraine vs aneurysm situation is onset. Migraine pain usually gives you some kind of runway. It may build over minutes, come with light sensitivity, nausea, or an aura, and feel like part of a pattern you recognize. A ruptured aneurysm usually does the opposite. It arrives suddenly and violently.
The question to ask first
Ask yourself: Did this headache peak almost immediately?
That question matters more than trying to score your pain or compare it with past attacks. People often get confused because migraines can be severe, disabling, and dramatic. Severity alone doesn't tell you enough. Speed of onset does.
Practical rule: A headache that becomes the worst pain you've felt within moments needs urgent medical attention, especially if it also comes with neck stiffness, fainting, seizure, confusion, weakness, or trouble speaking.
Why so many people second-guess themselves
Migraine can involve nausea, vomiting, visual symptoms, dizziness, and sensitivity to light. Those overlaps can make a dangerous headache easy to rationalize away as “just a bad one.” That's why it helps to think less about how miserable it feels and more about whether it behaves like your usual migraine pattern.
If the pattern is dramatically different, treat that change seriously. If you ever have a sudden severe headache, headache with fever or stiff neck, neurological changes, or headache after head injury, seek immediate medical care.
Understanding the Two Conditions Fundamentally
Migraine and aneurysm can both involve head pain, but they are not the same kind of problem. One is a neurological disorder. The other is a structural blood vessel problem.
How migraine works as a neurological condition
Migraine is more than a bad headache. It's a brain-based disorder that often unfolds in phases. As noted in this overview of migraine and aneurysm distinctions, migraines are characterized by a four-phase cycle: prodrome, aura, the headache phase, and postdrome.
Here's what those terms mean in plain language:
- Prodrome: early warning signs that can show up 24 to 48 hours before the head pain. You might notice mood changes, food cravings, fatigue, or that something just feels “off.”
- Aura: temporary neurological symptoms, often visual, that can last 5 to 60 minutes. Some people see zigzags, flashing lights, or blind spots. Others feel tingling or have trouble finding words.
- Headache phase: the pain itself, often throbbing, often one-sided, and commonly worse with activity. This phase typically lasts 4 to 72 hours.
- Postdrome: the “migraine hangover,” which can leave you drained, foggy, or unusually sensitive for up to 48 hours after the pain eases.
Not everyone gets every phase. Some people never have aura. Others mostly notice the prodrome and headache. That variation is normal in migraine.
How an aneurysm differs
A brain aneurysm is a weak, bulging spot in an artery in the brain. An unruptured aneurysm may cause no symptoms at all. A ruptured aneurysm is different. It causes bleeding around the brain, called a subarachnoid hemorrhage, and that is an emergency.
The symptom pattern is very different from a standard migraine pattern. A ruptured aneurysm is known for a thunderclap headache, meaning the pain reaches maximum intensity in less than one minute. It may also come with sudden loss of consciousness, seizures, or focal neurological changes such as slurred speech or one-sided weakness, which are not standard migraine features in the usual presentation described by major headache organizations and summarized in the same Brain Ritual review.
Migraine tends to unfold. A ruptured aneurysm tends to strike.
That basic difference helps everything else make more sense.
The Critical Difference Onset and Pain Profile
If you remember only one part of this article, remember this one. The clearest difference between migraine and a ruptured aneurysm is how fast the pain reaches its peak.
The fastest clue is timing
For many people with migraine, pain ramps up over a short period and then keeps developing. Verified clinical criteria indicate that migraine pain typically escalates over 15 to 30 minutes, while a ruptured aneurysm presents as a thunderclap headache that spikes to maximum intensity within seconds, under 1 minute. Headaches with sudden peak intensity are 95% predictive of subarachnoid hemorrhage rather than migraine.
That's a huge distinction. You can think of it as dimmer switch vs light switch.
If you want a separate overview of how early migraine patterns can appear before the main attack, Relief has a useful guide on recognizing migraine warning signs.
How the pain usually feels different
Migraine pain is often described in ways that many readers will recognize:
- Throbbing or pulsating
- Often one-sided
- Commonly paired with light sensitivity, sound sensitivity, or nausea
- Sometimes preceded by aura
Aneurysm-related rupture pain tends to be described differently:
- Explosive or thunderclap
- Sudden, maximal, and unfamiliar
- Often not neatly one-sided
- Not a gradual “my usual migraine is building” feeling
That said, don't rely on just one adjective. People use different words for pain. One person says “pounding.” Another says “pressure.” Another says “my head felt like it burst.” Language is imperfect. The timing is more reliable than the description.
Why confusion happens anyway
A bad migraine can still be intense enough to scare you. It can also bring vomiting, visual symptoms, and sensitivity to light. That overlap is why many people focus on the wrong clue. They ask, “Was it severe?” when they need to ask, “How did it begin?”
Severe migraine is common. Instantly maximal headache is not a normal migraine pattern and needs emergency evaluation.
If a headache feels different from your established migraine pattern, especially if the difference is suddenness, don't wait it out at home.
When to Seek Immediate Emergency Care
This is the section to be firm. A sudden severe headache with neurological symptoms is not something to monitor casually. It needs emergency attention.
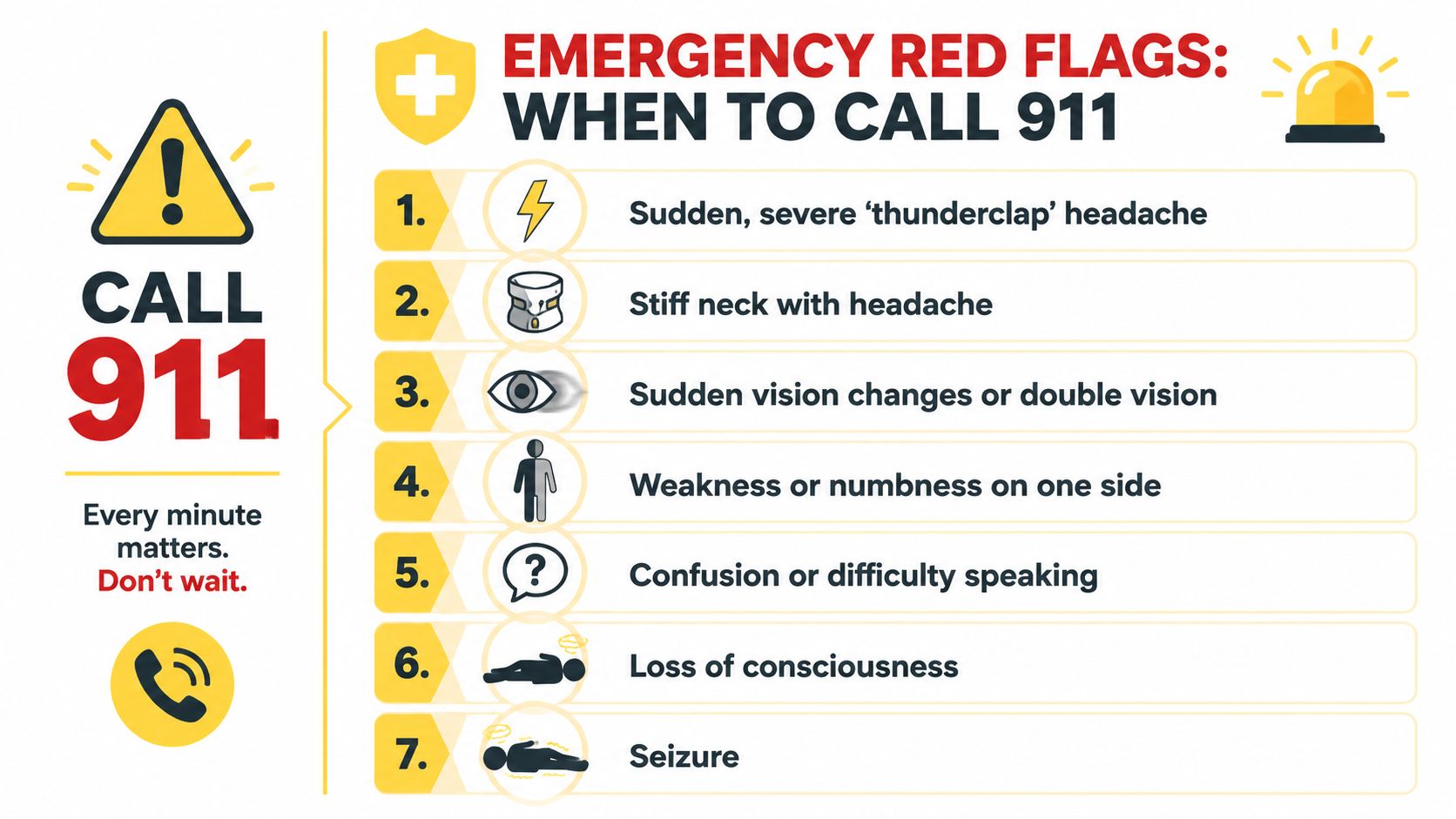
Here's a visual checklist first.
Red flags that are not typical migraine features
Verified emergency data show that subarachnoid hemorrhage has a triad of emergency markers with high specificity above 90% that are absent in migraine: sudden loss of consciousness, seizures, and severe neck stiffness. The presence of either seizure activity or immediate loss of consciousness is a 99% positive predictor for subarachnoid hemorrhage.
Call emergency services or go to the ER immediately if a headache comes with any of these:
- Thunderclap onset: pain hits maximum intensity within moments
- Loss of consciousness: even brief fainting is a major red flag
- Seizure activity: this is not part of a standard migraine picture
- Stiff neck with headache: especially if it appears suddenly and severely
- Sudden vision changes: such as double vision or a dramatic visual shift
- Confusion or trouble speaking: slurred speech, trouble understanding, or acting unusually confused
- One-sided weakness or numbness: weakness in an arm, leg, or one side of the face
- Headache after head injury: this always deserves urgent medical assessment
- Headache with fever and stiff neck: another emergency pattern that needs prompt evaluation
For readers who sometimes experience facial or sensory symptoms during migraine and want to better understand what fits a migraine pattern and what doesn't, this Relief article on headache with facial tingling may help with general symptom awareness.
A short video can also help reinforce what emergency symptoms look like in real life:
What to do in the moment
If this happens to you or someone near you:
- Call emergency services right away.
- Don't drive yourself if you're impaired, faint, confused, or having neurological symptoms.
- Tell the clinician exactly how it started. “It reached maximum intensity immediately” is useful information.
- Don't assume it's your usual migraine if the pattern is clearly different.
This is not overreacting. It is the correct response to a potentially life-threatening event.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Do Migraines Increase Your Risk for an Aneurysm
This fear often underlies the symptom question. If you live with migraine, you may wonder whether the condition itself means you're at higher risk for a brain aneurysm.
What current evidence says clearly
The reassuring part comes first. Migraines do not cause aneurysms. Having migraine does not mean you are causing a weak spot to form in a blood vessel, and it does not mean a migraine attack is turning into an aneurysm.
The nuance is that recent research found a modest statistical association in some groups. A 2024 meta-analysis in Neurology found that people with frequent migraines, defined as 4 or more per month, had a 1.3x higher risk of harboring an unruptured aneurysm compared with people without migraines, but no causal link was established.
That distinction matters. Correlation is not causation.
What that finding means in real life
Population-level research can identify patterns without proving that one condition creates the other. In practical terms, this means:
- It doesn't mean your migraines are damaging your brain arteries
- It doesn't mean every person with frequent migraine needs to fear an aneurysm
- It doesn't mean a typical migraine attack should be treated as a hidden bleed
It does mean that simple yes-or-no articles often leave out important nuance. “No connection at all” is too simplistic. “Migraines lead to aneurysms” is also wrong.
The balanced takeaway is this: migraine itself is not an aneurysm warning label, but unusual headache changes still deserve medical attention based on symptoms, not fear alone.
If your migraines have become more frequent, more disabling, or noticeably different, bring that up with your clinician. That conversation is about good migraine care and appropriate evaluation, not panic.
Navigating Diagnosis and What to Expect
A hospital visit for a severe headache is stressful partly because of uncertainty. Knowing the basic path can make it less intimidating.
What usually happens if doctors suspect bleeding
If a clinician is worried about a ruptured aneurysm or another brain bleed, the process is usually fast and focused on ruling out danger first. Doctors often start with an urgent CT scan of the head to look for bleeding.
If they still need more information, they may order additional testing such as a lumbar puncture or vascular imaging like a CT angiogram. Those tests can sound scary, but the reason is straightforward: when the concern is bleeding around the brain, speed and clarity matter.
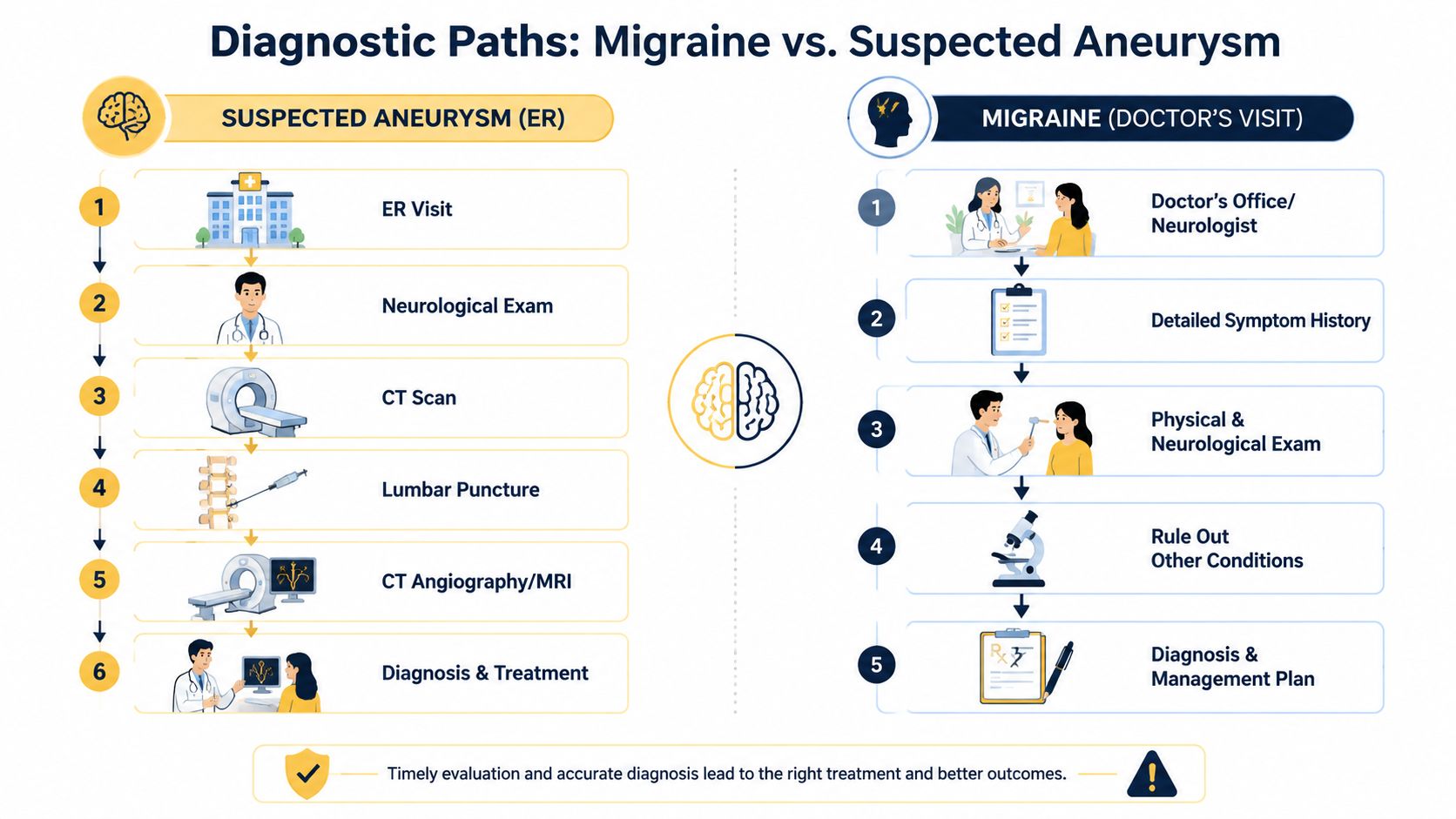
How migraine is usually diagnosed
Migraine diagnosis usually looks very different. In a clinic or neurology visit, the key tool is your history. A clinician wants to know:
- How your attacks begin
- Whether you get aura
- How long they last
- What symptoms travel with the pain
- How often they happen
- What has changed over time
They'll also do a neurological exam and may order tests if something about your story suggests a secondary cause.
If you've ever struggled to describe your symptoms accurately in an appointment, tools that help organize your history can make that easier. Relief's migraine or headache quiz is one example of a simple way to sharpen the conversation before you see a clinician.
The safest diagnostic mindset is simple: doctors rule out the dangerous things first, then sort out the chronic pattern.
That approach can feel alarming in the moment, but it is reassuring. It means the system is designed to catch emergencies before settling on a migraine diagnosis.
Using Your Knowledge for Proactive Migraine Management
The more clearly you know your own migraine pattern, the less helpless you feel when head pain starts. That doesn't remove every fear, but it gives you a better baseline. You can tell the difference between “this is miserable but familiar” and “this is new, abrupt, and not behaving like my migraines.”
That kind of pattern awareness matters because migraine is a condition you live with repeatedly. Tracking onset, aura, nausea, light sensitivity, pain location, duration, and after-effects can help you notice what's normal for you and what isn't.
A simple log can be useful if you include:
- Start pattern: gradual build or sudden onset
- Neurological symptoms: aura, numbness, speech trouble, confusion
- Pain description: throbbing, pressure, explosive, one-sided, diffuse
- Associated symptoms: nausea, light sensitivity, neck pain, vomiting
- Recovery pattern: postdrome, fatigue, brain fog, return to baseline
That record helps with both safety and care quality. It can also reduce anxiety because you're not relying on memory during a painful episode.
Relief can help you track symptoms, triggers, timing, and changing patterns in one place, so you have a clearer picture of what your migraines usually look like and when something may need more urgent attention.