
Most migraines in pregnancy are not dangerous, and up to 80% of women with a history of migraine improve during pregnancy, especially later on. But any new, severe, or different-feeling headache, especially with blood pressure at or above 140/90 or after 20 weeks, needs immediate medical evaluation to rule out problems such as preeclampsia.
If you're reading this with one hand on your forehead and the other on your phone, you're probably asking a very specific question: is this my usual migraine, or is this something I should act on right now? That anxiety is understandable. Pregnancy changes your body quickly, and migraine symptoms can overlap with normal pregnancy symptoms in frustrating ways.
Migraine is common during the reproductive years. One BMJ review reported a prevalence of 18.6% among women aged 20 to 64 and noted that recorded prevalence increased from 2000 to 2018, which helps explain why this question comes up so often during pregnancy (BMJ review on migraine prevalence and pregnancy patterns). At the same time, a migraine history before pregnancy isn't just a comfortingly familiar diagnosis. A Harvard report on a Neurology study found that prepregnancy migraine was linked to a 17% higher risk of preterm delivery, a 28% higher rate of gestational hypertension, and a 40% higher rate of pre-eclampsia compared with no migraine (Harvard report on migraine history and pregnancy risks).
That doesn't mean every migraine in pregnancy is an emergency. It does mean you shouldn't brush off a headache just because you've had migraines before.
Table of Contents
- The practical difference between aura and danger signs
- Migraine Aura vs. Potential Emergency Symptoms
- Lifestyle steps that actually help
- Non-drug options during an attack
- Over-the-counter options
- Prescription treatment decisions
Introduction
Pregnancy can make a familiar disease feel unfamiliar. A person who has managed migraine for years may suddenly wonder whether their usual nausea, light sensitivity, or visual symptoms still count as "normal" now that they're pregnant.
The hard part isn't usually identifying a classic emergency. Identifying a sudden, crushing headache as bad news is typically straightforward. The harder question is the gray zone: a headache that still feels somewhat like migraine, but not quite. Maybe the pain is in a new location. Maybe the aura is lasting longer than usual. Maybe you're vomiting more than you normally would, or your usual rescue routine isn't touching it.
Practical rule: In pregnancy, "different" matters almost as much as "severe."
That's because dangerous secondary headaches can initially look messy rather than dramatic. Public guidance often tells people to seek care for sudden severe headache, neurologic symptoms, or vision changes. That's correct, but it's incomplete. The practical problem is deciding when a known migraine has changed enough to stop self-managing and get evaluated.
A useful way to think about it is this: if the attack still matches your established pattern and improves with your usual supportive steps, it's more likely to be your migraine behaving like migraine. If the attack is new, first-ever, progressively worse, treatment-resistant, paired with high blood pressure, or clearly different from your normal pattern, you should stop assuming and get checked.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Understanding How Pregnancy Changes Migraines

Why attacks often improve
A common pregnancy headache question is whether a change in migraine frequency is reassuring or concerning. In many patients, migraine improves as pregnancy progresses, especially after the first trimester. I often see attacks become less frequent, less intense, or less tied to the hormonal swings that drove them before pregnancy.
The likely reason is hormonal stability. If your migraines used to cluster around your period, that pattern may ease once estrogen levels stop rising and falling in the usual monthly cycle. Some patients still have attacks, but the pattern becomes more predictable. Others improve only after the nausea and fatigue of early pregnancy settle.
Relief is common, but it is not universal.
That matters because a patient who knows, "My migraines usually start with neck tightness, then light sensitivity, then one-sided pain," has a reference point. During pregnancy, that reference point helps more than any single symptom. The practical question is not only, "Do I still get migraines?" It is, "Does this attack still behave like my migraine, or has the pattern changed in a way that deserves a second look?"
For a deeper look at cycle-linked patterns and prevention strategies, ReliefMigraine's guide to hormonal migraine prevention is a useful companion read.
What a familiar migraine pattern looks like
A familiar migraine often keeps its usual sequence, even if one part softens or drops out. The prodrome can still show up as fatigue, food cravings, irritability, neck discomfort, or trouble focusing. Aura remains a reversible neurologic symptom, such as visual changes, tingling, or temporary language trouble. The postdrome is the drained, foggy phase after the pain improves.
Pregnancy can blur that picture. Nausea may be worse, but nausea alone does not make a headache dangerous. Auras may happen without much headache pain, which can feel unsettling if you are used to a more obvious migraine attack. Sleep disruption, dehydration, missed meals, and iron deficiency can also change how an attack feels, even when the cause is still migraine.
This is the gray area patients struggle with most. A migraine can be different without being dangerous. At the same time, pregnancy is not a setting where a clearly changed headache should be brushed off.
The most reassuring pattern is a headache that still resembles your established attacks in timing, symptoms, and response to simple measures like rest, hydration, food, and your approved treatment plan. I get more concerned when the pattern loses that internal consistency. Examples include pain in a completely new location, an aura that lasts longer than your usual aura, vomiting that is far beyond your typical attack, or a headache that keeps building instead of following its normal course.
A first-ever migraine-like headache in pregnancy deserves more caution than the same symptom outside pregnancy. So does a migraine history that suddenly becomes much less predictable. The reason is practical. Early preeclampsia or another secondary headache disorder may not announce itself with a dramatic textbook presentation at the start. It may begin as a headache that feels close to your usual migraine, but not close enough.
That is why I tell patients to judge the whole pattern. One overlapping symptom rarely settles the question. A recognizable migraine pattern is somewhat reassuring. A changed pattern lowers the threshold to call your obstetric clinician and ask whether you need to be seen.
Red Flag Symptoms That Require Urgent Attention
If you have any of the symptoms below, don't wait to see whether this turns into "just a migraine."
The symptoms that should change your plan immediately
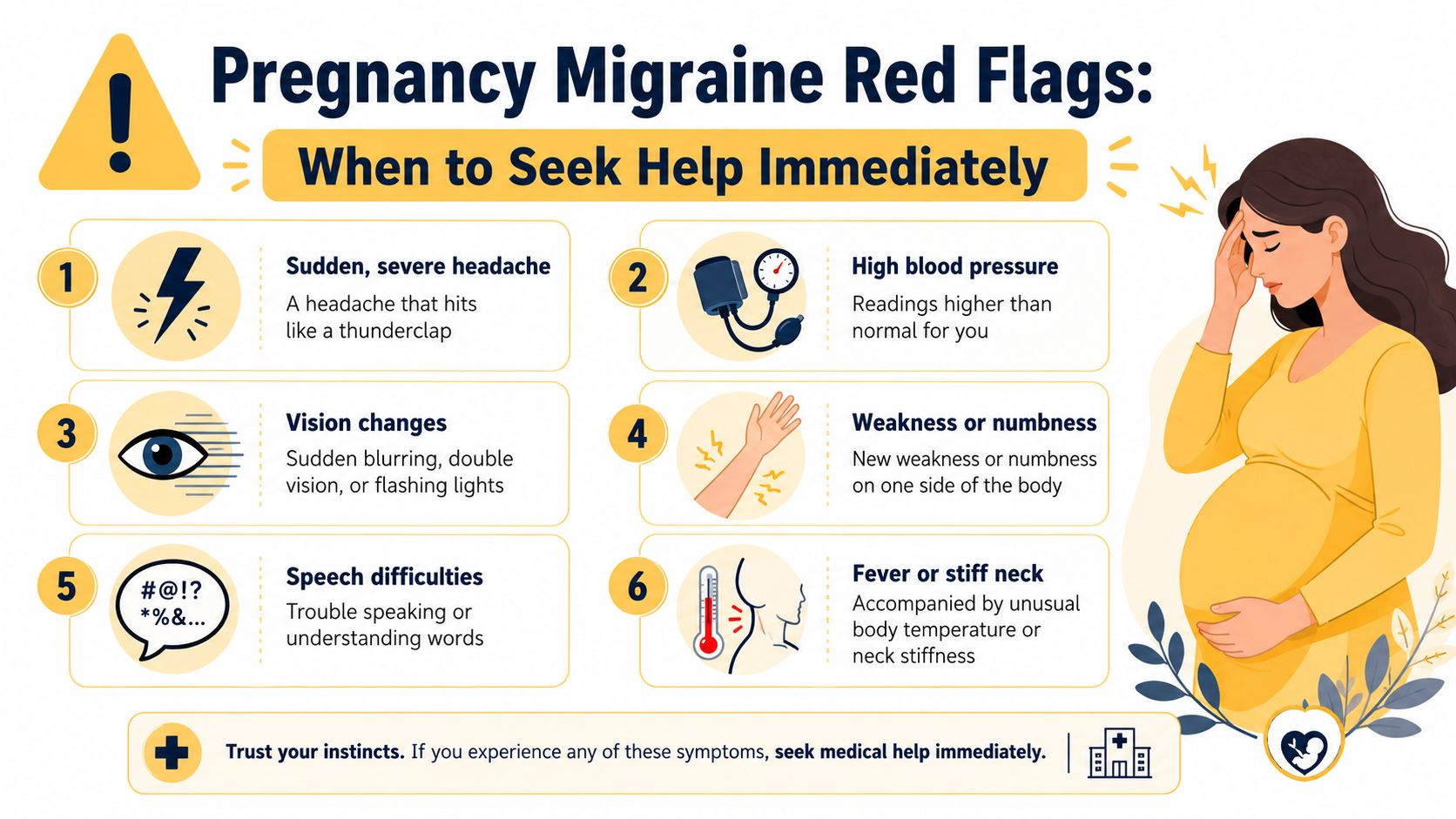
A pregnancy headache needs immediate evaluation when it has high-risk features. Key red flags include a headache that is new or different from your typical migraine, has a sudden or thunderclap onset, or is accompanied by fever, neck stiffness, rash, severe vomiting, visual changes, or blood pressure of 140/90 or higher in pregnancy (pregnancy migraine red flag guidance).
Use this checklist:
- New headache pattern. You've had migraine before, but this one feels unlike your usual attacks in quality, location, timing, or associated symptoms.
- Thunderclap onset. The pain peaks suddenly rather than building the way your typical migraine does.
- High blood pressure. If you know your reading is 140/90 or higher, don't talk yourself out of getting checked.
- Vision changes that feel wrong for you. Not your familiar aura. New blurring, major visual loss, or persistent visual disturbance needs urgent attention.
- Fever or stiff neck. A headache with these symptoms can point away from migraine.
- Severe vomiting or inability to keep fluids down. Dehydration can worsen migraine, but severe vomiting can also muddy the picture and delay needed evaluation.
- Neurologic symptoms. Weakness, numbness, trouble speaking, confusion, or trouble walking should be treated as an emergency.
- Headache after head injury. This always deserves prompt medical assessment.
- Headache that won't respond at all to your usual pattern of care. Refractory symptoms matter more in pregnancy.
Later in this section, this short video may help you review the warning signs visually:
What urgent really means
Urgent doesn't mean "mention it at your next prenatal visit." It means call your obstetric team now, go to labor and delivery if that's what you've been instructed to do, go to urgent obstetric triage, or go to the emergency department depending on local guidance and how severe the symptoms are.
A severe headache in pregnancy is not something to "watch overnight" if it's new, rapidly escalating, or paired with blood pressure elevation or neurologic symptoms.
What usually doesn't work is trying to force certainty at home. People often delay care because they're searching for the one symptom that proves it's dangerous. In reality, clinicians are taught to worry about new-onset or refractory headaches and any change in headache pattern, severity, or response to treatment when ruling out conditions like pre-eclampsia, stroke, or venous thromboembolism, as summarized in the earlier Harvard-linked report.
If you're not sure whether your symptoms cross the line, that uncertainty itself is part of the reason to call.
This article is for informational purposes and is not medical advice. Seek immediate medical care for sudden severe headache, headache with fever or stiff neck, neurologic changes, or headache after head injury.
Distinguishing Migraine Aura From a Neurological Emergency
The practical difference between aura and danger signs
Many people find themselves freezing here. They know they get aura. They also know stroke and preeclampsia can affect vision, sensation, and speech. The overlap is real, but the feel of the event is often different.
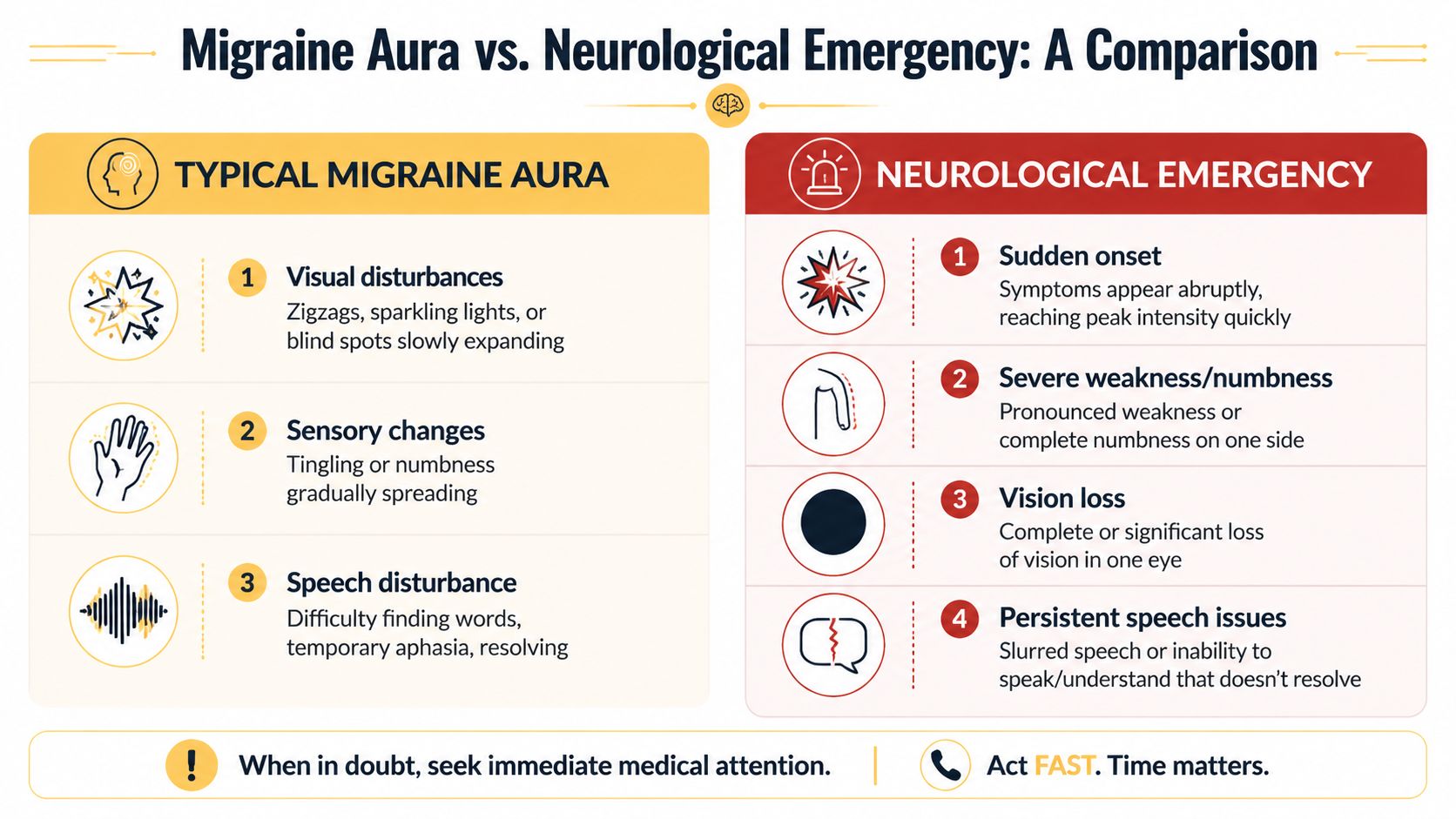
A typical migraine aura often adds symptoms before it takes them away. People describe shimmering lights, zigzags, sparkles, spreading tingling, or words that become briefly hard to find. The change often builds and moves.
A neurologic emergency more often causes a sudden loss of function. Vision may disappear rather than shimmer. An arm may become weak rather than tingly. Speech may become slurred or incomprehensible rather than briefly effortful.
That's not a perfect rule, and pregnancy isn't the time to gamble on self-diagnosis. But it is a useful starting point.
If facial tingling is part of what confuses your attacks, ReliefMigraine's article on headache with facial tingling can help you think more clearly about symptom patterns.
Migraine Aura vs. Potential Emergency Symptoms
| Symptom Type | Typical Migraine Aura | Potential Emergency (Seek Immediate Care) |
|---|---|---|
| Onset | Often develops gradually and feels like it unfolds | Appears abruptly or escalates very quickly |
| Visual symptoms | Shimmering lights, zigzags, sparkling shapes, expanding blind spots | Sudden major blurring, persistent vision loss, or a visual symptom that is entirely unlike prior aura |
| Sensory symptoms | Tingling or numbness that seems to spread | Pronounced numbness, weakness, or one-sided dysfunction |
| Speech symptoms | Temporary word-finding trouble that resembles your prior attacks | Slurred speech, inability to speak, or difficulty understanding language |
| Headache relationship | May be followed by a familiar migraine phase with light sensitivity, nausea, or typical pain pattern | May occur with severe blood pressure elevation, confusion, severe vomiting, or a very different headache quality |
| Recovery | Symptoms usually resolve in the way your previous attacks have resolved | Symptoms persist, worsen, or don't fit your established pattern |
A few practical questions help in the gray zone:
- Is this symptom part of my known pattern? If you've had visual aura many times and this episode behaves exactly the same way, that's more reassuring than a first-ever visual event.
- Is the symptom additive or subtractive? Sparkles and zigzags are different from a curtain of vision loss.
- Did it spread, or did it hit all at once? Gradual progression leans more toward aura. Sudden maximal deficit is more concerning.
- Did anything else change too? High blood pressure, swelling, severe vomiting, chest symptoms, or a much worse headache all lower the threshold for urgent evaluation.
When patients tell me, "It feels like migraine, but not my migraine," I take that seriously.
What doesn't help is trying to compare yourself to someone else's aura. Migraine types vary widely. Some people have visual aura. Others have sensory or language symptoms. Some have hemiplegic migraine or vestibular symptoms. The right comparison is always your current event versus your own baseline.
If this is your first-ever aura in pregnancy, or your aura is lasting longer than usual, more intense than usual, or paired with blood pressure issues or unusual neurologic symptoms, seek care promptly.
Safe Migraine Management Options in Pregnancy
Managing migraine in pregnancy is partly about symptom control and partly about reducing the chance that a manageable attack turns into an exhausting spiral of pain, vomiting, dehydration, poor sleep, and panic. The best plan is usually layered.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance before taking any medication during pregnancy.
Lifestyle steps that actually help
Basic measures sound small, but they matter more in pregnancy because your margin for feeling off is smaller.
- Hydration. If you're prone to nausea or vomiting, steady fluid intake matters more than heroic catch-up drinking later.
- Regular meals. Long gaps without food can make some people's attacks easier to trigger.
- Sleep rhythm. Consistent sleep usually helps more than trying to "make up" lost sleep in big chunks.
- Lowering overload. Bright light, strong smells, missed meals, travel, and stress can pile onto an already vulnerable day.
What doesn't work well is chasing every possible trigger at once. Pregnancy already limits your energy. Focus first on the few variables that clearly worsen your attacks, such as skipped meals, poor sleep, or dehydration.
Non-drug options during an attack
Non-drug treatment is often the first move because it has low downside and can make other steps more effective.
Try a combination rather than one isolated tactic:
- Dark, quiet environment. This can reduce photophobia and sensory overload.
- Cold pack. Many patients find a cold pack on the forehead, temple, or back of the neck more helpful than heat for migraine pain.
- Small amounts of fluid often. This is more realistic when nausea is active.
- Rest without fighting the attack. Pushing through screens, errands, or bright environments often prolongs the misery.
- Relaxed breathing or guided relaxation. Not because migraine is "just stress," but because muscle tension and panic can amplify pain.
The goal during an attack isn't to win points for productivity. It's to calm the nervous system and prevent escalation.
Over-the-counter options
Some over-the-counter medications may be used in pregnancy, but their appropriate use often leads to mixed messages from friends, internet lists, and old migraine habits.
Acetaminophen is commonly discussed as a lower-risk over-the-counter option in pregnancy. NSAIDs are a more complicated category and are often avoided later in pregnancy, especially in the third trimester. The right choice depends on your stage of pregnancy, your other medical issues, and your obstetric team's guidance.
A few rules keep people safer:
- Don't self-medicate based on your pre-pregnancy routine. A medication that was fine for you before pregnancy may not be the right choice now.
- Don't assume "over the counter" means harmless. Pregnancy changes the risk calculation.
- Don't combine products casually. Cold, sinus, and headache products may contain overlapping ingredients.
Prescription treatment decisions
Some prescription migraine treatments can still be considered during pregnancy, but those decisions belong with your obstetric clinician and, if possible, a clinician familiar with headache medicine. There is rarely one universal "best" prescription option.
A good plan separates two different jobs:
| Treatment goal | What that means in practice |
|---|---|
| Acute treatment | What you do when an attack starts |
| Prevention | What you do if attacks are frequent, disabling, or becoming harder to control |
That distinction matters because a medication that makes sense as an occasional rescue option may not be the right preventive strategy, and vice versa.
Ask your clinicians specific questions:
- Which medicines should I stop, continue, or avoid during pregnancy?
- What should I do if I can't keep fluids or food down?
- When do you want me to call for a headache that doesn't improve?
- If I have aura, what exact symptoms should send me straight in?
What usually works best is having the plan before the next bad attack. Trying to sort out medication safety while you're in severe pain and vomiting is hard.
Proactive Tracking and Communicating With Your Doctor
The safest way to handle migraines during pregnancy when to worry is to know your own baseline well enough to spot the headache that breaks the pattern. Memory is unreliable during pregnancy and even worse during a migraine. Written tracking is better.

What to write down every time
A useful migraine log doesn't need to be long. It needs to be specific.
Track these details:
- Start time and progression. Did it build gradually or hit suddenly?
- Pain features. Where was the pain, and did it feel like your usual migraine?
- Associated symptoms. Note nausea, vomiting, photophobia, phonophobia, aura, dizziness, weakness, numbness, speech issues, or anything unusual.
- What felt different. This is the single most useful line in many logs.
- Blood pressure if you have a reading. Especially important if the headache feels off-pattern.
- What you tried. Rest, fluids, cold pack, medication approved by your clinician.
- What happened next. Improved, stayed the same, worsened, or returned.
If you want a simple format to start with, ReliefMigraine's migraine log template is practical and easy to use.
When to call and when to go in
A simple decision rule helps:
| Situation | Best next step |
|---|---|
| Your usual migraine pattern, mild to moderate, improving with your normal safe routine | Contact your regular clinician if you need help refining management, especially if attacks are becoming more frequent |
| A headache that is different, unusually severe, or not responding the way your attacks usually do | Call your obstetric team the same day for advice |
| Sudden severe headache, neurologic symptoms, fever, stiff neck, head injury, or blood pressure at or above 140/90 in pregnancy | Seek immediate medical care |
Bring your notes to appointments. Clinicians make better decisions when they can see the pattern instead of trying to reconstruct it from memory. That is especially true when the question is not "Do you have migraine?" but "How has it changed?"
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Relief can make this process easier by helping you log symptoms, track patterns, and spot when an attack is different, so your conversations with your doctor are clearer and faster.