If you're tired of adding one more pill, one more supplement, or one more “try drinking more water” suggestion to your migraine routine, neuromodulation may be worth understanding. For some people, neuromodulation migraine treatment offers a non-drug option that uses electrical or magnetic stimulation to calm pain pathways involved in migraine, either during an attack or as prevention.
That doesn't mean it's simple, and it doesn't mean it's right for everyone. But it is a real treatment category with FDA-cleared devices, controlled studies, and a growing place in migraine care. This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
If you have a sudden severe headache, headache with fever or stiff neck, new neurological changes, or headache after a head injury, seek immediate medical care.
Table of Contents
- The main device types you may hear about
- Comparison of Common Neuromodulation Devices for Migraine
- What controlled studies have shown
Is There a Way to Treat Migraine Without More Pills
A lot of people reach this question after months or years of trying to “manage better” and still ending up sidelined by migraine. You may already know your triggers, carry acute medication, and still feel like your options are either incomplete or hard to tolerate.
Neuromodulation is different because it doesn't work like a drug. Instead of changing body chemistry, it uses a device to send targeted signals to nerves involved in migraine.
For some readers, that idea sounds futuristic. It isn't. Neuromodulation has moved from an experimental idea into a treatment category with multiple FDA-cleared options and a growing evidence base.
A useful way to frame it: this isn't a replacement for all other migraine care. It's another tool, especially relevant if you want a non-drug option, need to limit medication use, or want something you can combine with an existing plan.
You might also be exploring other newer treatment categories and wondering how they compare. If you're weighing device-based care against newer biologic approaches, this overview of CGRP monoclonal antibody treatment for migraine can help clarify how these paths differ.
What people usually want to know first
Most patients don't start with “What is the mechanism of action?” They ask practical questions:
- Will it help during an attack or is it only for prevention?
- Where do you put it on your body?
- What does it feel like when it's on?
- Can you still use medication if you need it?
- How do you choose between devices?
Those are the questions that matter in real life, especially when your brain is foggy and you're trying to function.
What Neuromodulation Is and How It Works for Migraine
Neuromodulation means using a device to influence nerve activity. In migraine, the goal is usually to calm or interrupt overactive pain signaling in the pathways involved in an attack.
Think of it as turning down a pain alarm
A simple analogy helps. Think of migraine as a pain alarm system that has become too easy to trigger and too loud once it starts. Neuromodulation doesn't “knock out” the whole system. It tries to turn down the volume on specific circuits.
Some devices use electrical stimulation. Others use magnetic pulses. Either way, the point is targeted input, not a whole-body medication effect.
That target matters. A review in Practical Neurology explains that external trigeminal nerve stimulation delivers inhibitory input through branches of the trigeminal nerve, and that signal then reaches the trigeminocervical complex, which is a key migraine-processing hub. The same review notes that single-pulse transcranial magnetic stimulation may interrupt cortical spreading depolarization, a leading proposed mechanism for migraine aura. You can read that discussion in this update on noninvasive neuromodulation devices for headache treatment.
Why the trigeminal nerve matters
If you've heard your neurologist mention the trigeminal nerve, that's because it's central to migraine biology. It's one of the main nerve pathways involved in head and face sensation, and it's fundamental to migraine pain processing.
Here's the plain-language version:
- Forehead devices often target branches of the trigeminal nerve.
- Neck devices may stimulate the vagus nerve.
- Arm devices can trigger remote pathways that affect pain processing.
- Back-of-head magnetic devices aim at brain signaling involved in migraine, including aura-related processes.
This is why neuromodulation can be used in more than one way. Some devices are meant for acute treatment, which means using them when an attack starts. Others are used preventively, meaning on a schedule to try to reduce how often migraine happens.
Migraine is not the same as a regular headache. It's a neurological condition that can involve aura, nausea, sensitivity to light or sound, dizziness, brain fog, and postdrome symptoms after the pain phase ends. Neuromodulation is aimed at those migraine-related nerve pathways, not just generic head pain.
Understanding Non-Invasive vs Invasive Approaches
The word “neuromodulation” can sound intimidating because it includes very different kinds of treatment.
On the skin versus under the skin
The cleanest way to understand it is this:
| Approach | What it means | Typical experience |
|---|---|---|
| Non-invasive | Device is worn, held, or placed on the skin | No surgery |
| Invasive | Device is implanted under the skin | Requires a procedure |
Non-invasive neuromodulation is often what is meant when discussing migraine devices. These are external tools. You wear them on the forehead, neck, arm, or head depending on the device.
Invasive neuromodulation involves a surgical procedure to place hardware under the skin. In migraine and related headache disorders, that approach is usually reserved for much more complex or refractory cases.
What most people with migraine actually discuss
For the average person seeing a primary care doctor, neurologist, or headache specialist, the conversation is usually about non-invasive options. That's good news if the idea of a procedure makes you uneasy.
These external devices are more like using a medical wearable than getting surgery. You control when you use them, how they fit into your day, and whether they belong in your broader treatment plan.
If you've looked into other procedure-based treatments, it can help to compare them with greater occipital nerve block options for migraine. A nerve block and a neuromodulation device are very different experiences, even though both involve nerve pathways.
Bottom line: when most patients ask about neuromodulation migraine treatment, they're usually asking about external devices, not implanted ones.
A Guide to FDA-Cleared Neuromodulation Devices
Once you start searching, the device names blur together fast. The easiest way to sort them is by where they go and what job they're meant to do.
Early in your research, a visual comparison helps: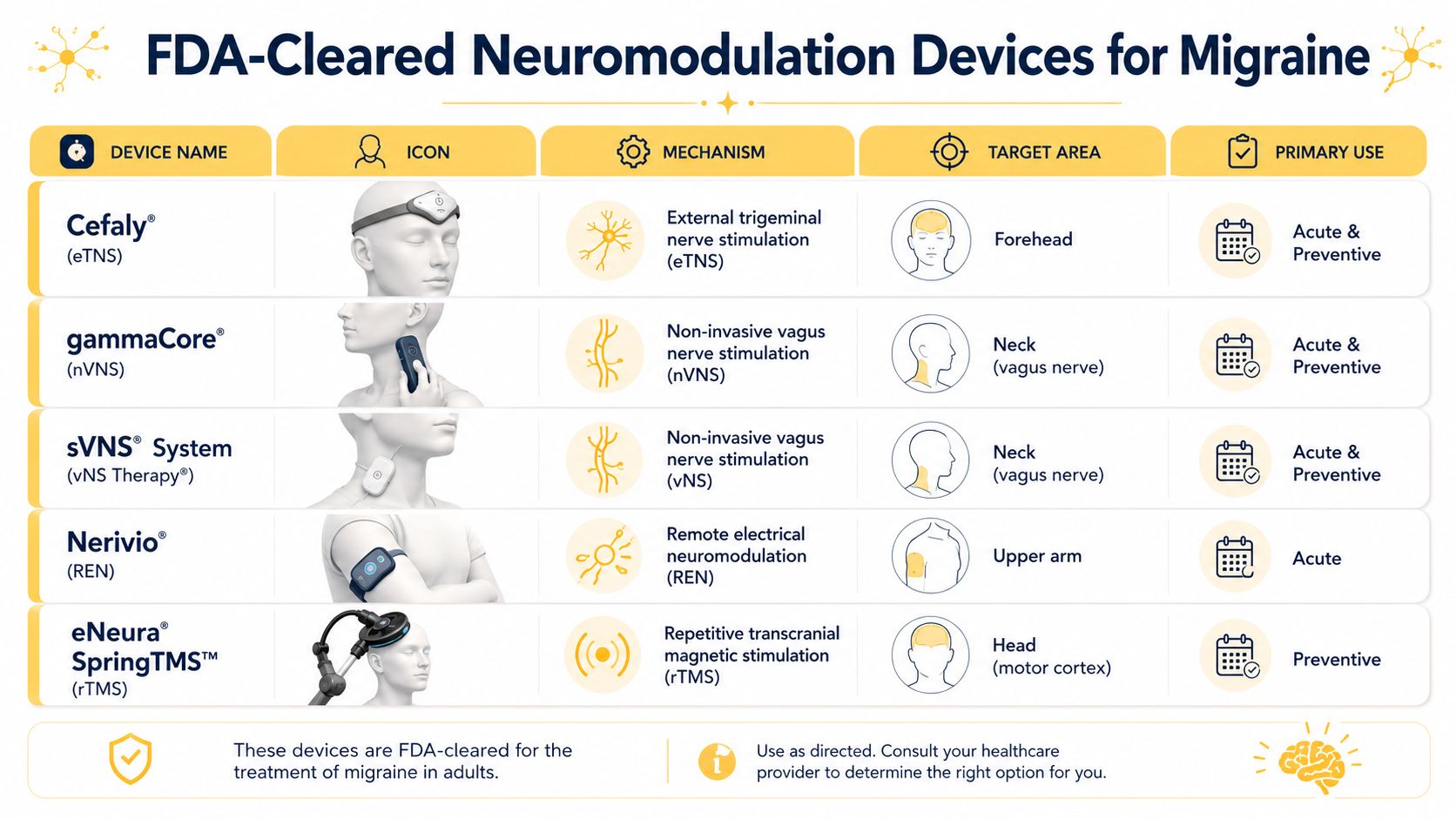
The main device types you may hear about
Cefaly is an external trigeminal nerve stimulation device used on the forehead. In plain terms, it targets trigeminal nerve branches near the forehead. People often describe this class of stimulation as tingling, buzzing, or a gradually building sensation on the skin. It's used for acute treatment and prevention.
Nerivio is a remote electrical neuromodulation device worn on the upper arm and controlled through a smartphone. That arm placement surprises people at first because it doesn't touch the head. But the goal is still migraine-related pain modulation through remote nerve signaling. It's used for acute treatment and prevention.
SAVI Dual is a single-pulse transcranial magnetic stimulation device placed on the back of the head. Instead of a buzzing electrical feel on the skin, magnetic stimulation is often experienced more like a brief tapping or pulse. This device is used for acute treatment and prevention.
A short demonstration can make the category feel less abstract:
gammaCore is a non-invasive vagus nerve stimulation device applied to the neck. The vagus nerve has broad roles in autonomic and pain-related signaling. This device is used for acute treatment and prevention.
Relivion MG is an external combined occipital and trigeminal neurostimulation headset. It stimulates both occipital and trigeminal nerve regions and is used for acute treatment.
HeadaTerm 2 is a TENS forehead device used for prevention.
Comparison of Common Neuromodulation Devices for Migraine
| Device Type | Target Nerve | Placement | Primary Use | Sensation |
|---|---|---|---|---|
| Cefaly eTNS | Trigeminal nerve branches | Forehead | Acute and preventive | Tingling or buzzing |
| Nerivio REN | Remote pain-modulation pathways | Upper arm | Acute and preventive | Adjustable electrical sensation |
| SAVI Dual sTMS | Brain signaling targeted by magnetic pulse | Back of head | Acute and preventive | Brief tapping or pulse-like sensation |
| gammaCore nVNS | Vagus nerve | Neck | Acute and preventive | Pulsing or vibrating sensation |
| Relivion MG eCOT-NS | Occipital and trigeminal nerves | Headset on head | Acute | Multi-point stimulation sensation |
| HeadaTerm 2 TENS | Forehead nerve pathways | Forehead | Preventive | Surface tingling |
What controlled studies have shown
This category isn't built only on theory. A 2019 review in The Journal of Neurology, Neurosurgery & Psychiatry found that non-invasive neuromodulation had already been studied in 10 primary-headache studies for noninvasive vagus nerve stimulation alone, including 4 acute migraine trials, 4 prevention trials, 2 acute cluster-headache trials, and 1 cluster-headache prevention trial. The same review reported 2-hour pain-free rates of 39% with single-pulse transcranial magnetic stimulation versus 22% with sham in one key acute migraine study, and 30.4% with noninvasive vagus nerve stimulation versus 19.7% with sham in another acute study, as described in this review of neuromodulation for primary headaches.
Those numbers don't mean every device works equally well, or that any one device will work the same way for you. They do show that this is a tested treatment area, not just a gadget trend.
Is Neuromodulation Effective and Who Can It Help
The honest answer is yes, for some people, and effectiveness depends heavily on the specific device and the job you're asking it to do.
Effectiveness depends on the device
One of the biggest misconceptions about neuromodulation migraine treatment is treating all devices as if they're interchangeable. They aren't.
A meta-analysis summarized by Practical Neurology found a real split in results. Remote electrical neuromodulation had pooled efficacy for acute migraine treatment with an effect size of 2.14 (95% CI 1.34-3.40), while supraorbital and percutaneous TENS and high-frequency repetitive transcranial magnetic stimulation over the primary motor cortex were found effective for prevention. The same summary noted that some other approaches did not show significant effects. That overview is available in this meta-analysis summary on neuromodulation for migraine treatment.
That matters because the right question isn't “Does neuromodulation work?” It's “Which device has evidence for the kind of migraine problem I'm trying to solve?”
Who tends to consider it
Neuromodulation often comes up for people who fit one or more of these patterns:
- You want a non-drug option. Maybe you prefer to minimize medication when possible.
- You can't tolerate some medications well. Side effects can limit even effective treatments.
- You need another tool. Some people use devices alongside lifestyle changes and medication, not instead of them.
- You want an option tied to timing. If your attacks have an early warning pattern, an acute device may fit that pattern well.
- You have aura or specific symptom patterns. Mechanism can matter when discussing which device to try.
Some devices may help best as a rescue tool early in an attack. Others make more sense if your main goal is prevention. Matching the tool to the problem is where most of the value comes from.
Safety discussions are important too. In general, these devices are often described as having reasonable evidence and low-risk profiles, but individual suitability still matters. People with implanted medical devices or certain other conditions may need extra caution, and your clinician should review the device instructions and your health history with you.
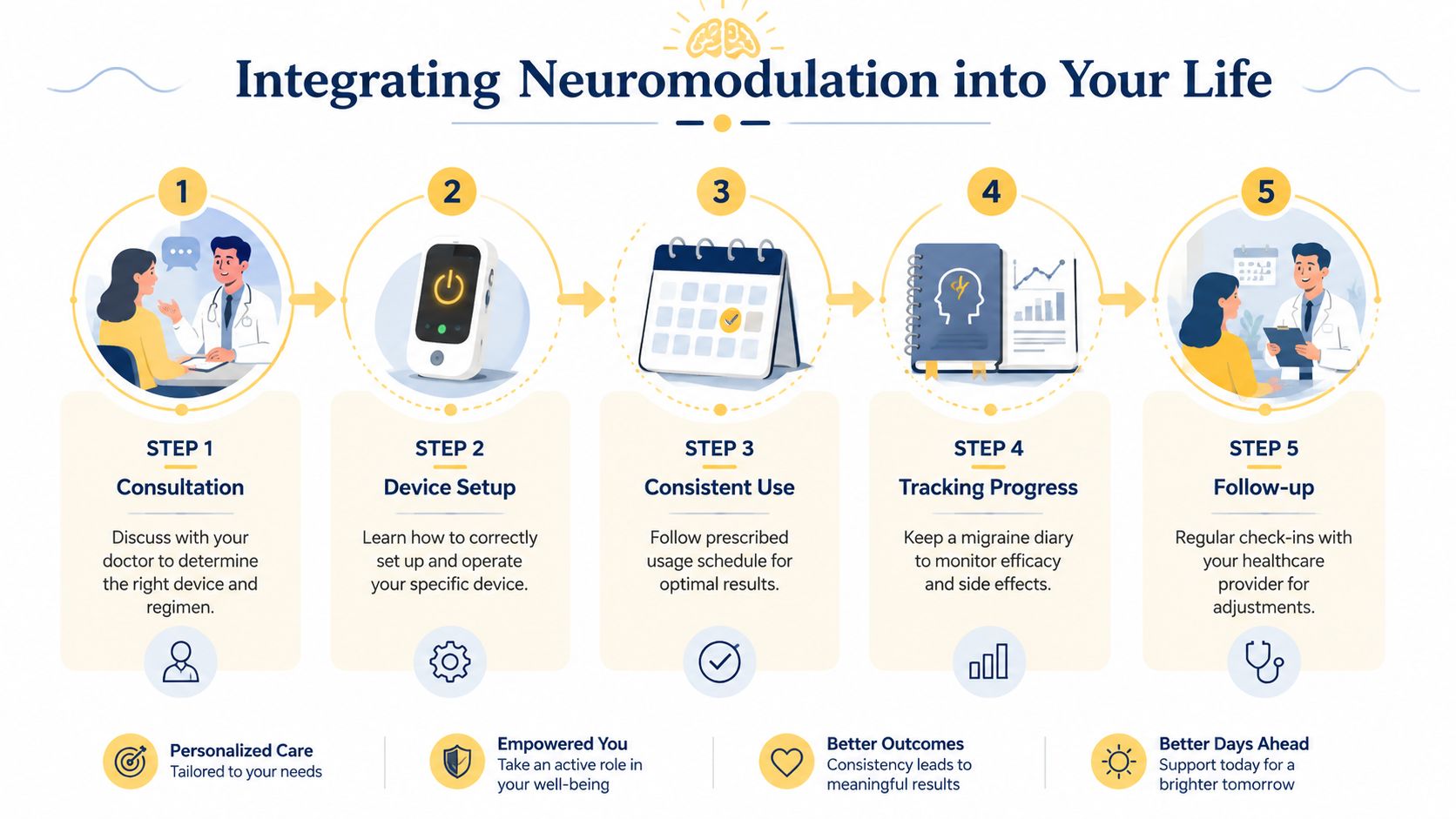
Your Practical Guide to Using Neuromodulation
The point where people usually get stuck is not on the science, but on the daily-life question: How would I use this?
A recent review points out that multiple FDA-cleared options now exist, but head-to-head evidence and clear selection rules are still limited. That gap is exactly why choosing based on aura, attack timing, and prevention versus rescue use needs a thoughtful discussion with your clinician, as noted in this review of non-invasive neuromodulation for primary headache disorders.
How to think about acute versus preventive use
A simple framework helps.
If your biggest problem is stopping attacks once they begin, ask about a device with an acute indication. These are often used at the first sign of migraine, which might be pain, aura, photophobia, nausea, or that hard-to-describe “I can tell one is coming” feeling.
If your biggest problem is how often migraine happens, ask about preventive use. Preventive neuromodulation usually works more like a routine than a rescue. That means consistency matters.
If both are true, your doctor may discuss a device that can be used in both ways, or how a device could fit alongside medication rather than replace it.
A related option some people also explore is a TENS machine for headache relief, especially when they're trying to understand how nerve stimulation feels in practice.
Questions to bring to your appointment
Bring specifics, not just “I've heard about neuromodulation.”
- My attacks start with: aura, neck pain, nausea, light sensitivity, or sudden pain.
- My main goal is: fewer attacks, better early stopping, or less reliance on medication.
- My migraine pattern is: episodic, frequent, chronic, menstrual-related, or vestibular features.
- I need something that fits: workdays, travel, parenting, screen-heavy days, or unpredictable schedules.
- I already use: acute medication, preventive medication, or non-drug strategies.
Practical rule: ask your doctor, “Based on my pattern, would you prioritize a device for acute use, prevention, or both?”
A few realistic expectations help:
- Timing matters. If a device is meant for early use, waiting too long may reduce your chance of benefit.
- Technique matters. Placement and proper use aren't minor details.
- Consistency matters. Preventive approaches usually need routine use.
- Tracking matters. You need a way to notice whether attack timing, intensity, or recovery is changing.
Common Questions and Your Next Steps
The most common remaining questions aren't about nerve anatomy. They're about real life.

What about pregnancy adolescents and special cases
This is an area where people need nuance, not blanket reassurance. A recent review notes that non-invasive neuromodulation is being investigated for vestibular migraine and comorbid depression, and that some devices have age-specific clearances, including for ages 12 and older, with one later update noting expanded pediatric clearance to ages 8+. The same review also notes that for pregnancy and breastfeeding, there still isn't enough information to confirm safety. You can see that discussion in this review of non-invasive neuromodulation in migraine and special populations.
So if you're pregnant, trying to conceive, breastfeeding, managing vestibular symptoms, or asking about a child or teen, don't assume the answer is automatically yes or no. Ask for device-specific guidance.
What to track before you decide
Cost and insurance coverage are practical barriers for many people. Coverage varies, device access varies, and the “best” option on paper may not be the most realistic option for your day-to-day life.
Bring a short record of:
- Attack timing such as morning, afternoon, overnight, or around your cycle
- Early symptoms such as aura, photophobia, nausea, dizziness, or neck pain
- Frequency pattern including whether attacks are clustered or spread out
- What you've already tried and whether the problem was side effects, poor fit, or limited benefit
- Your goal which might be reducing attack frequency, treating sooner, or adding a non-drug option
The more clearly you can describe your pattern, the easier it is for a clinician to match you with a device category instead of guessing.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Relief can help you walk into that conversation with better data. With Relief, you can track attack timing, symptoms, triggers, and patterns over time so you and your clinician can make a more informed decision about whether a neuromodulation device fits your migraine plan.