If you're reading this while one eye has gone blurry, dark, or filled with shimmering light, the fear makes sense. An ocular migraine in one eye can happen, but the more precise term is retinal migraine, and the first practical question is whether the visual change is in one eye or whether it only seems that way because the disturbance is affecting your visual field.
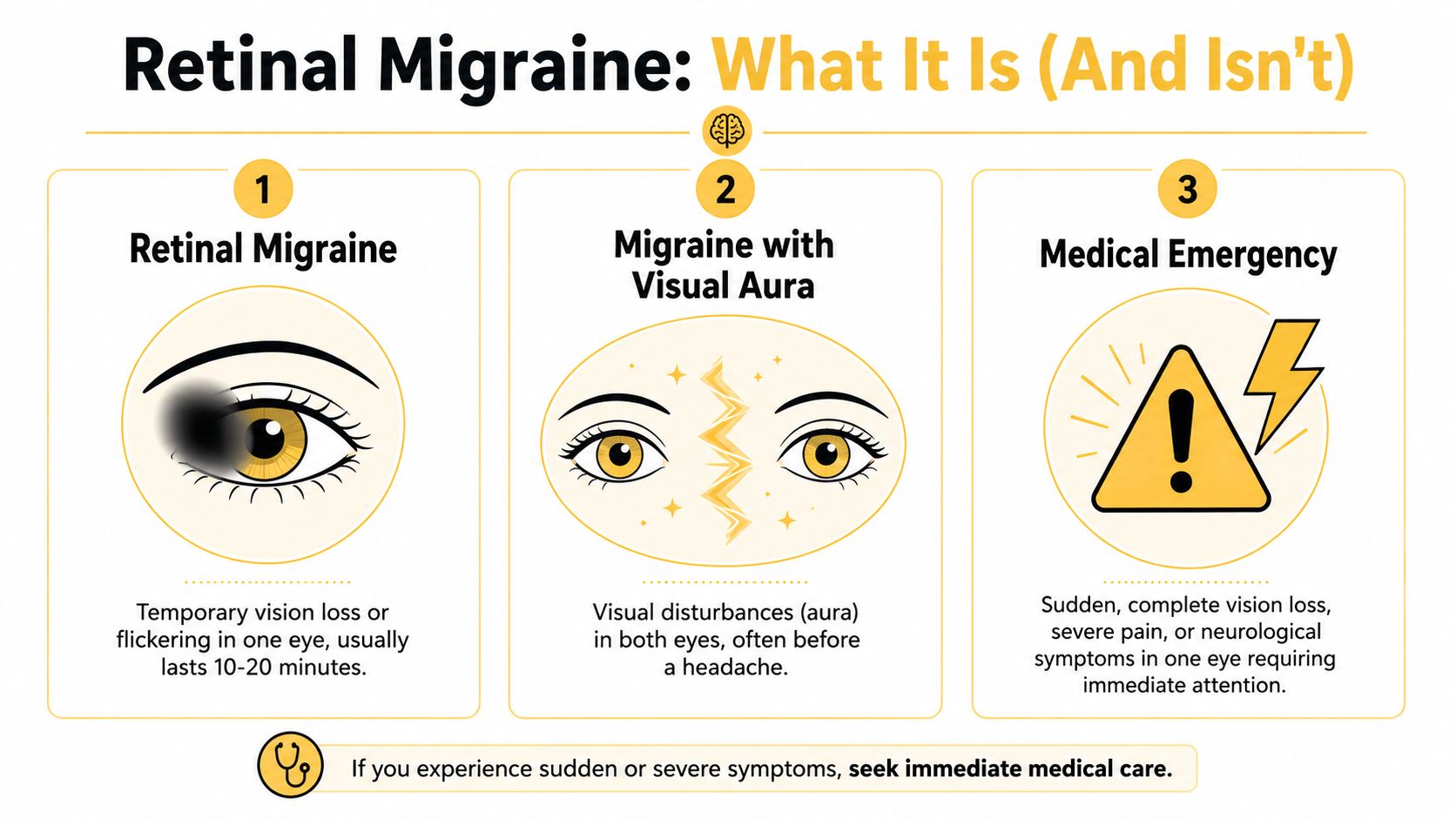
That distinction matters. A retinal migraine is a migraine event with strictly monocular visual symptoms such as a blind spot, temporary vision loss, or zigzagging shimmering lights in one eye, while the more common migraine aura usually affects both eyes because it comes from brain-based visual processing changes, as explained by Cleveland Clinic's overview of ocular migraine. This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
Table of Contents
Understanding One-Eyed Vision Changes
What the term really means
When people say “ocular migraine,” they often mean several different things. In clinic, that creates a lot of confusion, because some people are describing migraine with aura, some are describing silent migraine, and some are describing a true retinal migraine.
Retinal migraine is the term that fits vision changes in only one eye. Those changes can include a blind spot, dimming, shimmering, zigzagging lights, or temporary loss of part or all of vision in that eye. If you're also trying to sort out whether this is headache-free aura, this guide to silent migraine symptoms and patterns can help with the broader migraine picture.
Why one-eye symptoms feel so alarming
It feels alarming because your brain reads sudden visual loss as a threat. That reaction is appropriate. Vision changes in one eye deserve careful attention, even when migraine is part of the story.
Practical rule: If you can tell the symptom is happening in only one eye, take it seriously and don't brush it off as “just a headache.”
A common explanation is blood vessel spasm affecting the retina rather than the visual cortex. That means the mechanism is different from the classic aura many migraine patients know well. The result is a symptom that can look dramatic, even if it later resolves.
Migraine is not the same thing as a headache. A migraine is a neurological condition that may include aura, nausea, light sensitivity, sound sensitivity, and head pain. A headache is one symptom that may or may not show up.
Retinal Migraine vs Visual Aura and Emergencies
Visual symptoms are where many people get stuck. They know they've had migraine before, but this episode feels different because only one eye seems affected. That's exactly when a simple self-check can help.
Use the cover-one-eye test during the attack
The most useful real-time check is the cover-one-eye test. During the visual event, cover one eye and then the other.
- If the disturbance is present only when one specific eye is open, that supports a distinctly monocular problem and raises concern for retinal migraine or another eye-related cause.
- If the pattern seems visible no matter which eye is covered, that points more toward visual aura, which usually comes from the brain's visual pathways rather than the eye itself.
Mayo Clinic notes that 99% of people with migraine aura report visual symptoms in both eyes. That's why this test is so helpful in the moment.
Here's a short explainer to reinforce the distinction before you compare the patterns below.
How retinal migraine differs from aura and emergencies
Use this table as a quick sorting tool, not a diagnosis.
| Pattern | What it usually feels like | One eye or both | What to do |
|---|---|---|---|
| Retinal migraine | Blind spot, dimming, flicker, shimmering, or temporary vision loss that seems confined to one eye | One eye | Stop what you're doing, get somewhere safe, and arrange medical evaluation, especially if it's new or changing |
| Migraine with visual aura | Shimmering zigzags, sparkles, expanding pattern, or missing area in the visual field | Usually both eyes or one side of the visual field | Rest, reduce visual stimulation, and discuss with your clinician if it's new, frequent, or unusual |
| Emergency eye or brain event | Sudden major vision loss, shower of floaters, flashes, severe eye pain, weakness, numbness, speech change, or a very different severe headache | May start in one eye or come with other neurological symptoms | Seek urgent medical care right away |
A retinal migraine can overlap with migraine symptoms, but there's a reason many clinicians won't assume that's the answer on first pass. One-eye visual loss can also overlap with retinal detachment, blocked blood flow, or a stroke-related problem. If you're worried your symptoms might signal something more dangerous, this comparison of migraine vs aneurysm warning patterns is another useful safety read.
If the symptom is new, unusually intense, or paired with weakness or speech trouble, don't keep testing yourself at home. Get urgent help.
What works here is pattern recognition plus caution. What doesn't work is assuming every flashing light or blind spot is “just migraine” because you've had migraine before.
Symptoms and What to Do During an Attack
A one-eye visual episode is frightening. Patients often tell me their first thought is, "Am I losing vision for good?" That fear makes sense, and it is exactly why the first few minutes should be used for safety and quick observation, not guesswork.
How an attack often unfolds
Many attacks start suddenly. Part of the view in one eye may look gray, washed out, blurred, or blocked by a dark spot. Some people notice flickering or shimmering near the center of vision. Others notice that words disappear while reading or that faces look incomplete on one side.
A retinal migraine usually affects one eye only and then clears. The episode may be brief, but during the attack it can feel much longer. Vision often fades, holds for a short period, then gradually returns. Headache may follow, but not always.
One practical detail matters here. During the attack, cover one eye, then switch and cover the other. If the disturbance stays present only when one specific eye is open, that supports a true one-eye problem. If the pattern seems visible no matter which eye is covered, the source is more likely visual aura from the brain's visual system rather than the eye itself. That distinction is not a diagnosis, but it is very useful information to document and report.
What to do in the moment
Start with safety.
- Stop driving or using machinery: Pull over or stop the task as soon as you can do so safely.
- Get to a stable, low-stimulation space: Sit or lie down somewhere with less glare and less visual strain.
- Do the cover-one-eye test: Cover the right eye, then the left, and note whether the visual change stays in one eye.
- Check the clock: Write down when it started and when it begins to improve.
- Record what you saw: Note whether it was a dark patch, dimming, flashing, shimmering, blurring, or missing area.
- Note associated symptoms: Headache, nausea, light sensitivity, neck pain, or unusual fatigue can help your clinician sort out the pattern.
- Log possible triggers: Heat, dehydration, skipped meals, poor sleep, altitude change, and shifts in barometric pressure are worth tracking if episodes recur.
I tell patients to resist the urge to keep testing the eye every few seconds with a phone screen or by trying to read small text. That usually increases stress and light sensitivity without adding useful information.
There is a trade-off during an attack. Observation helps, but repeated self-checks can make you more anxious and less safe. A brief, structured note is better than constant monitoring.
If you have had similar episodes before and they resolve in the usual pattern, rest in a dim room and avoid driving until vision is fully back to normal. If this is the first episode, if the pattern has changed, or if recovery is incomplete, arrange medical assessment even if the vision returns.
A simple attack log can make future care much more precise. Record the date, start time, which eye was affected on the cover-one-eye test, how the symptom looked, how long it lasted, whether headache followed, and what was happening that day. In clinic, those details often do more to clarify the diagnosis than the label a patient was given years earlier.
This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
When to Seek Emergency Medical Help
A one-eye visual episode can feel frightening fast. The hardest part in the moment is knowing whether you are dealing with a migraine pattern that needs prompt follow-up or an eye or brain emergency that needs care now.
Use the cover-one-eye test once, early in the attack, then make a decision. If the visual change disappears no matter which eye you cover, the source is more likely in the brain's visual system, which fits visual aura more than a retinal event. If the disturbance stays present only when one eye is open, treat that as a true one-eye symptom until a clinician proves otherwise.
Time matters here. nidirect guidance on retinal migraine advises urgent assessment if vision symptoms last more than 60 minutes, begin for the first time after age 50, or occur without the headache pattern you usually get. In practice, I also advise urgent evaluation for any first episode of one-eye vision loss, even if it improves, because retinal migraine is a diagnosis made only after more dangerous causes have been considered.
There is a real trade-off. Watching for the pattern can help you describe what happened. Waiting too long can cost valuable treatment time if the episode is a retinal tear, retinal artery problem, stroke-related visual loss, or another urgent condition.
Get emergency help now if the vision loss is sudden and dark, if part of your vision is missing like a curtain, if new floaters or flashes appear, or if the visual change comes with weakness, numbness, trouble speaking, chest pain, severe eye pain, or the worst headache of your life.
If episodes keep recurring and emergency causes have been ruled out, discuss a prevention plan rather than relying on reassurance alone. Options may include trigger tracking, pressure-change awareness, and in some cases migraine prevention medication options.
Red flags that need urgent care
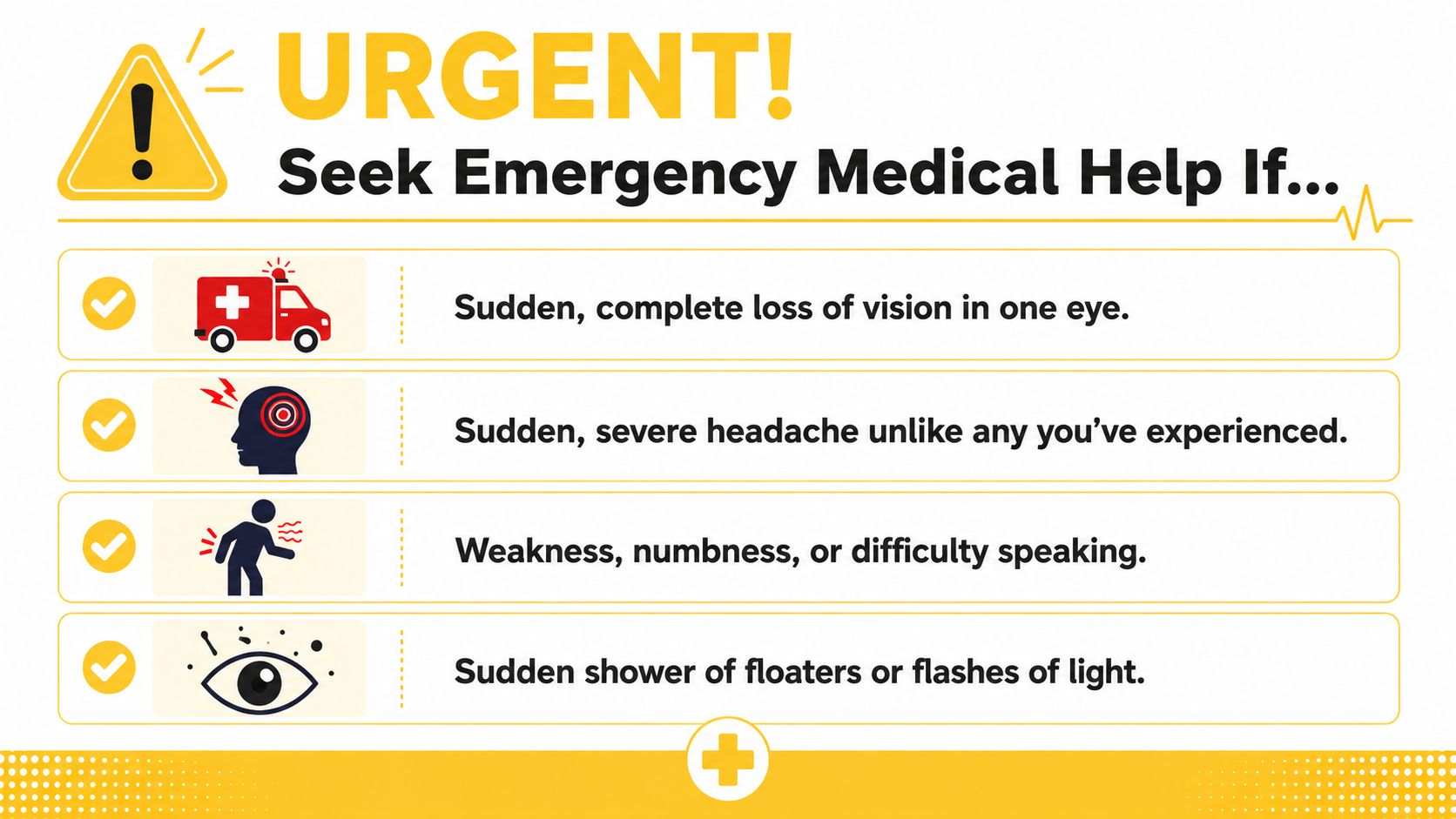
Some migraine symptoms are disruptive. Others are red flags. If you have any of the signs below, stop self-managing and seek immediate medical care.
- Vision loss that lasts longer than 60 minutes
- Visual symptoms that happen without a headache when that's not your usual pattern
- A first episode that begins after age 50
- Sudden severe headache unlike your usual migraine
- Headache with fever or stiff neck
- Neurological changes such as weakness, numbness, confusion, or difficulty speaking
- Headache after head injury
- Sudden shower of floaters or flashes of light
- A curtain-like shadow or persistent loss of vision
Why waiting can be risky
Retinal migraine can be mistaken for emergencies, and emergencies can be mistaken for retinal migraine. That's a significant danger.
The same nidirect guidance on retinal migraine warns that permanent vision loss is a documented risk and that immediate evaluation is critical if symptoms persist beyond 60 minutes, occur without a headache, or begin after age 50. One-eye visual changes may also need urgent evaluation to rule out stroke or retinal detachment.
New one-eye vision loss is not something to “watch for a few days.” It needs prompt assessment.
If your headache is sudden and severe, or comes with fever, stiff neck, weakness, or speech difficulty, seek emergency care immediately. This article is for informational purposes and is not medical advice. Consult a healthcare provider for personalized guidance.
How to Prevent Future Retinal Migraines
Prevention starts after the episode, when you can look at the pattern without the panic. The most useful plan usually combines diagnosis, trigger work, and, for some people, preventive treatment.
What clinicians usually look at
A clinician will usually want a careful history first. They'll ask what you saw, whether it was just one eye, how long it lasted, whether headache followed, and whether the pattern is stable or changing.
They may also examine the eye and retina to rule out causes that migraine can mimic. That part matters. Good prevention depends on being confident about what you're preventing.
Prevention that tends to help
For people with frequent retinal migraines occurring more than 4 days per month, this ophthalmic migraine overview notes that preventive management prioritizes calcium channel blockers such as nifedipine or verapamil because they target vascular spasm. It also highlights lifestyle measures like hydration and stress management, and mentions FL-41 tinted lenses as a non-drug option for light-triggered symptoms.
That doesn't mean one intervention works for everyone. It means prevention usually works best when you separate it into categories:
Lifestyle approaches
Regular hydration, steadier sleep, and reducing obvious visual or stress overload can lower the chance of some attacks.Over-the-counter options
These may help the headache phase for some people, but they don't fix the underlying vasospasm involved in retinal migraine.Prescription prevention
A clinician may discuss preventive medication when episodes are frequent, disruptive, or risky. No single prescription is the “best” choice for every patient.Emerging and non-drug tools
FL-41 lenses may help if light is a clear trigger. Some people also ask about non-invasive devices used in broader migraine care, especially when standard approaches haven't helped enough.
If preventive treatment is on the table, it helps to review a broader guide to migraine prevention medication options before your visit so you can ask better questions.
Environmental patterns worth tracking
A lot of migraine advice stays generic. “Manage stress” and “drink water” are useful, but they don't explain why one day is fine and the next day starts with a visual event in one eye.
Harvard Health points out that retinal or ocular migraine may stem from blood vessel issues in the eye or brain, and it highlights environmental links such as barometric pressure and humidity as important correlates in migraine patterns in its article on when vision problems are actually migraine attacks. That's worth paying attention to if your attacks seem to cluster around storms, pressure swings, or muggy days.
Try tracking these details for each episode:
| What to log | Why it matters |
|---|---|
| Time of onset | Helps you compare symptoms against weather and daily routines |
| Which eye was affected | Confirms whether the event is truly monocular |
| Visual pattern | Blind spot, dimming, shimmer, or complete loss can guide diagnosis |
| Headache and other migraine symptoms | Helps separate retinal migraine from aura-only patterns |
| Context | Sleep, dehydration, stress, bright light, altitude, smoking exposure, or hormonal shifts may matter |
| Environment | Barometric pressure, humidity, air quality, and sudden weather changes can reveal patterns over time |
What works is tracking your repeatable pattern. What doesn't work is relying on generic trigger lists and assuming every commonly named food or habit applies to you.
Discussing Your Symptoms with a Clinician
Many migraine patients arrive at appointments feeling like they need to prove what happened. That's especially common after a one-eye visual event, because it may be over by the time you're examined.
What to bring to the appointment
Bring a short record that answers the questions your clinician will need.
- What you saw: Was it a blind spot, dark patch, shimmer, zigzag line, or complete dimming?
- Which eye it affected: If you used the cover-one-eye test, say so.
- How long it lasted: Use the most honest estimate you can.
- What came with it: Head pain, nausea, photophobia, phonophobia, dizziness, or no headache at all.
- How often it happens: A rough count is better than “sometimes.”
- What was happening around it: Sleep disruption, dehydration, stress, bright light, altitude exposure, smoking, hormonal shifts, or weather changes.
A simple note on your phone is enough if it's clear. The best symptom logs are short, specific, and repeated consistently.
Questions worth asking
A productive appointment usually gets better when you ask direct questions.
- Do my symptoms sound monocular, or more like visual aura?
- What conditions are you trying to rule out besides migraine?
- Do I need an eye exam or additional testing?
- What should make me seek emergency care next time?
- Would preventive treatment make sense if these episodes continue?
- What should I track between now and the next visit?
Clear tracking changes the conversation. It turns “I had something weird happen” into a symptom history a clinician can actually use.
You don't need to sound medical. You just need to be precise. That often leads to faster recognition of patterns, fewer assumptions, and a better plan.
If you want an easier way to log attacks, spot patterns, and track environmental signals like barometric pressure, Relief can support that process without replacing medical care.